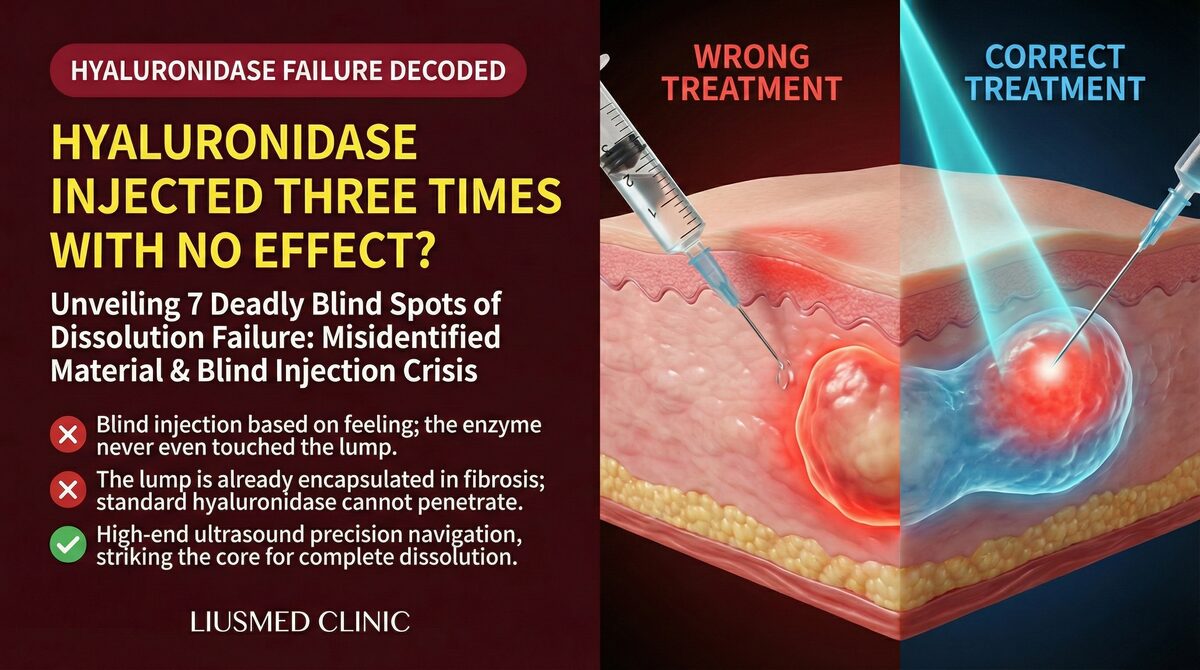
One of the most frustrating presentations in a revision clinic is a patient arriving with records of three or more hyaluronidase injections — yet the hyaluronic acid (HA) filler remains, the nodule persists, and the asymmetry is still clearly visible. Hyaluronidase is the standard enzymatic tool for dissolving HA, so why does it sometimes simply fail?
This article documents the seven most common clinical scenarios where hyaluronidase falls short, explains the ultrasound appearance of residual HA, explores why dissolving displaced filler can actually worsen asymmetry, and describes the structural reason why encapsulated HA is impervious to enzymatic treatment. Finally, it outlines when ultrasound-guided single-pinhole physical extraction offers more precise and predictable results.
Understanding the fundamental difference between dissolving and revising is the first step toward choosing the right approach.
"Hyaluronidase Isn't Working": Seven Clinical Scenarios Where Dissolution Fails
Hyaluronidase breaks down the cross-linker structure within HA filler molecules. In theory, with sufficient dose and accurate delivery, virtually any HA can be degraded. In practice, "failed dissolution" is far more common than expected. Here are the seven most important reasons.
1. Highly Cross-Linked Brands Require Substantially Higher Doses
Different HA filler brands vary enormously in their resistance to hyaluronidase. Juvéderm and RHA4, which use Vycross high-molecular-weight cross-linking technology, are among the most resistant HA fillers to hyaluronidase — in vitro they require substantially higher enzyme volumes and longer exposure to degrade than biphasic HA products, which dissolve more readily (PMC11093662).
Many clinics use a standard dose of 30–50 U, which is severely inadequate for highly cross-linked products. Insufficient dosage is not evidence that the enzyme is "ineffective"; it means the target was never reached.
Key insight: The most resistant commercial HA fillers require substantially higher doses than are commonly administered. When dissolution fails, the first question should be whether adequate enzyme actually reached the filler.
2. Encapsulation: A Fibrous Capsule That Blocks the Enzyme
When HA filler persists in tissue over time, a low-grade chronic foreign-body response can prompt fibroblasts to deposit collagen around the filler mass, forming a thin fibrous capsule. Once this capsule forms, hyaluronidase must penetrate the capsule wall before it can reach the HA — this is one of the primary structural reasons why repeated hyaluronidase injections produce diminishing results. See the encapsulation section below for the full mechanism.
3. Deep Placement in Subcutaneous Fat Compartments
HA injected into deep fat compartments (such as the deep cheek fat pad or supraperiosteal plane) is physically inaccessible to hyaluronidase injected at a superficial level. Ultrasound-guided direct injection into the filler mass significantly improves dissolution success rates for deeply placed HA.
4. Incorrect Dilution or Injection Technique
Over-concentrated enzyme, placement away from the filler mass, or surface injection rather than intra-filler injection all reduce efficacy substantially. Published guidance emphasises direct injection into the filler mass rather than superficial application, as the latter was found significantly less effective (PMC11733830).
5. Local Fibrosis From Repeated Injection Cycles
Repeated cycles of dissolution and re-filling can induce mild local fibrosis, restricting the diffusion pathway of subsequent enzyme injections. This is the histological basis for the clinically observed phenomenon of "harder to dissolve with each attempt."
6. Permanent Filler Mistaken for HA
Some "hyaluronic acid" injected in certain countries or clinics from earlier eras contains PAAG (polyacrylamide gel) or silicone, against which hyaluronidase has no effect whatsoever. If there is any uncertainty about what was originally injected — particularly for injections performed abroad or before 2010 — ultrasound characterization is essential before attempting enzymatic dissolution.
7. Irregular Distribution of Displaced HA
Once HA has migrated from its original injection site, its distribution is irregular and wider than intended. Hyaluronidase injected into one zone diffuses outward unpredictably, potentially dissolving well-placed filler nearby while leaving the displaced portion largely intact — creating new asymmetry rather than correcting it.
"Not Completely Dissolved": What Residual HA Looks Like on Ultrasound
After hyaluronidase treatment, patients often assess the result by external appearance or palpation — but accurate assessment of residual filler requires ultrasound imaging.
On ultrasound, HA filler presents as a distinctive hypoechoic (dark) mass with a well-defined boundary. Even when a nodule feels softer or asymmetry appears marginally improved, ultrasound frequently demonstrates substantial residual HA in the deeper tissue planes, particularly when encapsulation has formed a fibrous wall around a filler pocket that remains largely intact.
Key insight: "It feels softer" is not the same as "the HA is gone." Only ultrasound can objectively confirm the location and volume of residual filler — which is why Dr. Ta-Ju Liu uses ultrasound evaluation both before and after every hyaluronidase treatment.
Why Encapsulated Filler Resists Dissolution provides detailed ultrasound case illustrations including images typical of residual HA after multiple hyaluronidase injections.
The companion piece The Myth of Complete HA Absorption presents evidence that highly cross-linked HA persists in tissue far longer than manufacturer timelines suggest — with some cases showing identifiable residual on ultrasound five to ten years post-injection.
Filler Displacement Revision: Why Simple Dissolution Can Worsen Asymmetry
Displacement (migration) occurs when filler moves from its original injection plane due to gravity, muscle movement, or improper initial placement depth. This is fundamentally different from overfilling — the problem is not total HA volume but location: it is somewhere it should not be.
Three Risks of Dissolving Displaced HA
Imprecise targeting. Hyaluronidase spreads outward from its injection point in a zone that cannot be controlled. When displaced HA sits adjacent to well-placed filler, the enzyme will dissolve both — creating a new depression where none existed before.
Asymmetry can worsen. Both sides of the face rarely have identical displacement patterns or volumes. Broad dissolution often corrects one side more than the other, introducing or exacerbating asymmetry that was not present prior to treatment.
No objective endpoint. Without ultrasound, there is no way to confirm when dissolution is "complete," how much residual remains, or where the filler boundary now sits. The clinician and patient are guessing.
The Correct Approach to Displacement Revision
Ultrasound mapping first — confirm the exact position, depth, and volume of displaced HA before choosing a strategy: targeted local dissolution (for early, superficial displacement), or physical extraction from the original position (for deep displacement, encapsulated cases, or repeated failed dissolution).
For HA that has displaced into high-risk anatomical zones — such as the infra-orbital area, deep nasolabial fold, or periorbital region — physical extraction is more likely to achieve complete clearance and eliminate the risk of re-migration.
For a case-based discussion of asymmetry correction, see Filler Asymmetry After Injection: Assessment and Correction.
Encapsulation Makes Hyaluronidase Ineffective: Mechanism and Alternatives
Encapsulation is one of the most under-recognized and frequently misdiagnosed HA filler complications — because clinically it can appear nearly identical to simple residual HA. The key distinguishing feature is not the external appearance, but the ultrasound image.
What Is Encapsulation?
When HA filler persists in tissue for an extended period, the body's immune system mounts a chronic low-grade foreign-body response. Fibroblasts gradually deposit collagen around the filler mass, creating a thin fibrous capsule (several millimeters thick in advanced cases). On palpation, this presents as a firm, well-demarcated spherical or oval nodule — typically non-tender, non-erythematous, and immobile under pressure. This distinguishes it from early HA nodules that have not yet encapsulated and can often be displaced slightly with pressure.
Why the Enzyme Cannot Penetrate
Hyaluronidase is an enzyme molecule. While not exceptionally large, the dense collagen network of a fibrous capsule physically impedes its diffusion. The majority of enzyme injected outside the capsule is metabolized in surrounding tissue before it can penetrate to the HA mass within.
Key insight: Encapsulated HA does not fail to dissolve because hyaluronidase is ineffective against it — the enzyme cannot reach it. This structural barrier is why repeated high-dose injections produce consistently limited results. The problem is not dose; it is access.
Comparison of Treatment Approaches
← Swipe to see more →
| Hyaluronidase Only | Ultrasound-Guided Physical Extraction | |
|---|---|---|
| Capsule penetration | Difficult (collagen network impedes diffusion) | Capsule punctured directly; contents extracted |
| HA clearance confirmation | Cannot be visually confirmed | Real-time ultrasound monitoring |
| Effect on surrounding tissue | Adjacent normal HA may also dissolve | Precise targeting, minimal collateral disruption |
| Best for | Early, non-encapsulated, low cross-linked HA | Encapsulated, highly cross-linked, prior failed cases |
| Sessions typically needed | Multiple | One or few |
| Ultrasound guidance | Recommended but often omitted | Standard pre- and post-procedure |
Confirming Encapsulation
Ultrasound is the most reliable diagnostic tool. Encapsulated HA appears on ultrasound as a hypoechoic (dark) core with a clearly defined hyperechoic (bright) rim — often described visually as an "egg" shape. Palpation alone cannot reliably distinguish encapsulated from non-encapsulated HA, but the ultrasound image is diagnostic. Once encapsulation is confirmed, continued enzymatic dissolution offers very limited benefit and physical extraction evaluation is appropriate.
Physical Extraction of Hyaluronic Acid: The Clinical Logic of a Single Pinhole
Single-pinhole physical extraction is the minimally invasive approach used at this clinic for HA cases where dissolution has failed, encapsulation is confirmed, or displacement requires precise-position removal.
The Core Principle: See Before Treating
Physical extraction begins with seeing: ultrasound-guided localization of the HA's exact position, depth, extent, and capsule status before any instrument is placed. No instrument enters without ultrasound confirmation. This is the structural opposite of "inject hyaluronidase where it feels hard."
"See before treating" is not a slogan; it is the architectural principle of the entire treatment workflow. Ultrasound documentation at three time points — pre-procedure assessment, intra-procedure monitoring, and post-procedure confirmation — provides an objective record of what was found and what was removed.
Indications
Physical extraction offers advantages over hyaluronidase alone in these situations:
- Hyaluronidase has failed at least twice (encapsulation or high cross-linking suspected)
- Encapsulation confirmed on ultrasound (hyperechoic capsule rim visible)
- Displaced HA in a defined location requiring precise-position extraction
- Tyndall effect (a bluish-gray discoloration caused by superficially placed HA scattering light)
- Filler overfilling syndrome (FOS / pillow face) combined with encapsulation
Post-Procedure Recovery
Single-pinhole extraction uses a minimal puncture incision; post-procedure scarring is not typically visible. Local tissue depression is expected immediately post-procedure and usually resolves within 2–4 weeks as collagen remodeling and tissue rebound occur. A minority of cases require a small amount of structural fill (autologous fat or minimal HA) following extraction to restore contour; this is discussed during consultation.
For technical details on the extraction approach, see Physical Extraction Techniques for Filler Nodules.
FAQ
Q1: I've had three rounds of hyaluronidase and still have nodules. Is this definitely encapsulation?
Not necessarily — but three failed rounds is a strong clinical indicator. It may also reflect consistently insufficient dose for a highly cross-linked filler, or inaccurate injection placement. Ultrasound evaluation is the appropriate next step to determine whether a hyperechoic capsule rim is present before committing to further enzymatic treatment or switching strategy.
Q2: Is repeated hyaluronidase injection safe?
Hyaluronidase should be administered only after medical evaluation. Repeated injection cycles carry the risk of progressive local fibrosis, which makes subsequent dissolution increasingly difficult. If multiple rounds have produced minimal benefit, the priority should be reassessing the strategy — not simply increasing injection frequency.
Q3: My filler has migrated. Why not just dissolve all of it?
Because hyaluronidase cannot selectively dissolve only the displaced portion — it diffuses outward from the injection point and affects adjacent tissue, including well-positioned filler. The likely outcome of undifferentiated full dissolution is incomplete removal of the displaced filler combined with new hollowing where filler was originally working well. Ultrasound mapping should precede any dissolution attempt in displacement cases.
Q4: Will physical extraction leave scars or permanent hollowing?
Single-pinhole extraction uses a minimal puncture that leaves no visible scar in the vast majority of cases. Post-extraction tissue depression typically resolves within 2–4 weeks. In cases where contour correction is needed after extraction, a small amount of structural fill may be placed — this is assessed during consultation and is an expected, plannable part of the treatment sequence.
Is Your Situation a Candidate for Dissolution or Revision?
If hyaluronidase has already failed, if filler has displaced, or if you suspect encapsulation, repeating the same injection one more time is unlikely to change the outcome. Precise diagnosis is the correct starting point.
Dr. Ta-Ju Liu provides full-face ultrasound assessment to objectively characterize filler location, depth, and capsule status, followed by a structured discussion of the most appropriate revision approach — targeted dissolution, physical extraction, or a sequenced combination of both.
Book a filler revision consultation →
Learn more about HA Filler Revision Services or visit the HA Filler Conditions Hub for a full overview of hyaluronic acid complications and their management.
This article is written by Dr. Ta-Ju Liu based on clinical practice and current medical literature, for educational purposes only. It does not constitute medical diagnosis or treatment advice. Each patient's situation is unique; please arrange an in-person consultation before making treatment decisions.
Editorial Review — Dr. Ta-Ju Liu