The Core Challenge of Filler Lump Extraction
"I've been to three different clinics. They all told me the lump couldn't be fully removed, or that I'd need open surgery with visible scarring." If this sounds familiar, you are not alone. Many patients arrive at FILLER REVISION after being told their filler lumps were untreatable — only to discover that with the right technique, complete extraction is absolutely possible.
The goal of minimally invasive filler lump extraction is to completely remove the foreign material while maximally preserving normal tissue. This requires precise localization, skilled technique, and deep understanding of different filler characteristics. This article explains professional extraction techniques and principles.
Types of Filler Lumps
Classification by Filler Material
← Swipe to see more →
| Filler Type | Dissolvable | Lump Characteristics | Removal Difficulty |
|---|---|---|---|
| Hyaluronic Acid | ✅ Yes | Soft, clear boundaries | Lower |
| Collagen | ❌ No | Medium firmness | Medium |
| Radiesse (CaHA) | ❌ No | White, granular | Medium-High |
| Collagen Stimulator | ❌ No | Hard, irregular | High |
| Silicone/Oil | ❌ No | Migrating, diffuse | Very High |
| PMMA (Polymethyl Methacrylate) | ❌ No | Permanent, encapsulated | Very High |
Classification by Problem Type
← Swipe to see more →
| Problem Type | Common Cause | Treatment Approach |
|---|---|---|
| Migrated lump | Post-injection displacement | Locate and extract |
| Overfilled lump | Excessive injection | Partial or complete removal |
| Inflammatory lump | Foreign body reaction | Anti-inflammatory then extract |
| Infected lump | Bacterial infection | Control infection first |
| Calcified lump | Long-standing presence | If minimally invasive extraction is not feasible after evaluation, surgical excision may be used |
Why Is Lump Extraction Difficult?
Technical Challenges
← Swipe to see more →
| Challenge | Explanation |
|---|---|
| Localization difficulty | Filler may migrate and diffuse, hard to determine extent |
| Unclear boundaries | Mixed with normal tissue, difficult to separate |
| Sensitive location | Face has important nerves and vessels |
| Secondary damage | Over-extraction causes depression |
| Residue risk | Incomplete removal leads to recurrence |
Difficulty Varies by Material
Difficulty from low to high:
Hyaluronic Acid (dissolvable)
↓
Radiesse (granules can be curetted)
↓
Collagen Stimulator (severe fibrosis)
↓
Silicone (migrating diffusion)
↓
PMMA (permanent encapsulation)
💡 Dr. Liu explains: "At FILLER REVISION, we've refined this technique through thousands of cases — matching each filler type to its optimal extraction approach. Hyaluronic acid can be dissolved first, Radiesse needs curettage, collagen stimulator requires careful separation of fibrotic tissue. No single method works for all cases, which is why material-specific expertise matters."
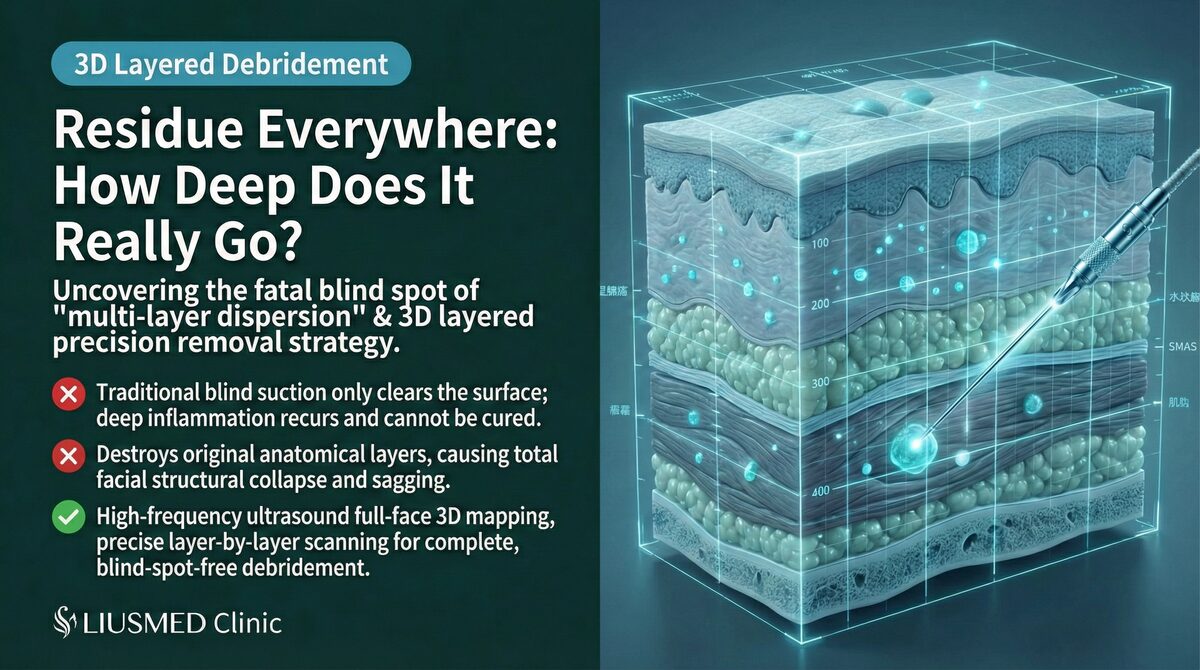
Ultrasound (Ultrasonography)-Guided Technology
Why Is Ultrasound Necessary?
← Swipe to see more →
| Advantage | Explanation |
|---|---|
| Precise localization | Real-time imaging shows filler location |
| Boundary identification | Distinguishes foreign material from normal tissue |
| Depth assessment | Understands filler depth and extent |
| Safe guidance | Avoids important vessels and nerves |
| Intraoperative monitoring | Confirms complete removal |
Ultrasound Characteristics of Different Fillers
← Swipe to see more →
| Filler | Ultrasound Features |
|---|---|
| Hyaluronic Acid | Hypoechoic, homogeneous |
| Radiesse | Hyperechoic, granular |
| Collagen Stimulator Lump | Mixed echogenicity, irregular |
| Silicone | Hyperechoic, "snowflake" phenomenon |
| Calcified Tissue | Strong echo, posterior shadow |
Precision Extraction Technique
Surgical Principles
- Minimal incision: Use minimally invasive incisions to reduce scarring
- Precise localization: Confirm position under ultrasound guidance
- Conservative excision: Remove only foreign material, preserve normal tissue
- Layer separation: Separate along tissue planes
- Confirm completeness: Ultrasound verification of no residue
Surgical Steps
Step 1: Pre-operative Assessment
← Swipe to see more →
| Item | Content |
|---|---|
| History taking | Filler type, injection time, clinic |
| Physical exam | Lump location, size, depth |
| Ultrasound exam | Precise localization and extent assessment |
| Treatment plan | Determine optimal extraction method |
Step 2: Anesthesia and Preparation
- Primarily local anesthesia
- Mark incision location
- Ultrasound preparation
Step 3: Pinhole Design
We use pinhole minimally invasive extraction, with pinhole size typically 1-2mm.
← Swipe to see more →
| Consideration | Design Principle |
|---|---|
| Hidden scar | Along skin lines or concealed areas |
| Close to lesion | Shorten operating distance |
| Adequate view | Ensure complete extraction possible |
| Minimal wound | Usually 1-2mm |
Step 4: Lump Extraction
Ultrasound localization → Pinhole entry → Find filler layer →
↓
Careful separation (preserve normal tissue) → Complete extraction →
↓
Ultrasound confirms no residue → Hemostasis → Suture
Step 5: Post-operative Care
- Pressure dressing
- Antibiotics for infection prevention
- Schedule follow-up
Extraction Strategies by Filler Type
Hyaluronic Acid Lumps
← Swipe to see more →
| Approach | Suitable Situation |
|---|---|
| Hyaluronidase injection | Mild irregularity, small area |
| Dissolve + curettage | Incomplete dissolution residue |
| Direct extraction | Encapsulated, hyaluronidase ineffective |
About Hyaluronidase:
- Can dissolve hyaluronic acid, but limited effect on encapsulated lumps
- Takes effect 24-48 hours after injection
- If ineffective, surgical extraction needed
Radiesse Lumps
← Swipe to see more →
| Characteristic | Approach |
|---|---|
| Granular | Primarily curettage |
| May spread | Need careful clearing of surroundings |
| Not dissolvable | Physical removal only |
Collagen Stimulator Lumps
← Swipe to see more →
| Characteristic | Difficulty |
|---|---|
| Stimulates tissue growth | Lump and normal tissue hard to distinguish |
| Severe fibrosis | Unclear boundaries |
| May continue growing | Requires complete removal |
Key Points:
- Complete excision of fibrotic tissue
- Ultrasound confirmation of extent
- Post-op monitoring for recurrence
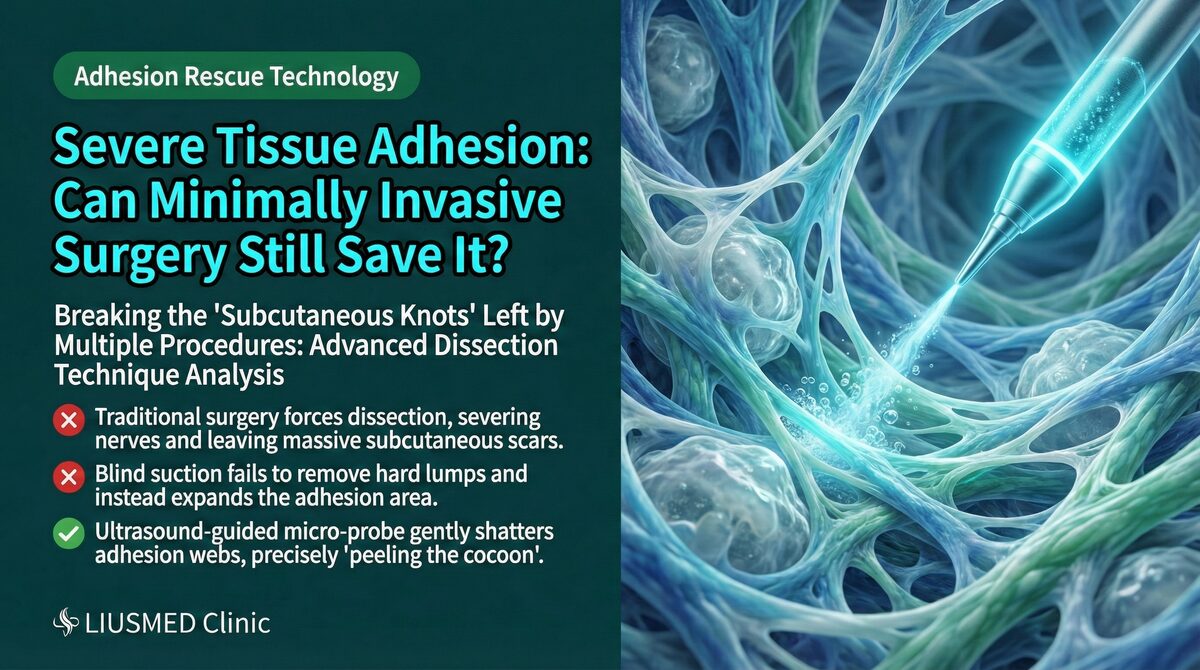
Silicone/Silicone Oil
← Swipe to see more →
| Characteristic | Extremely Difficult |
|---|---|
| Migrating diffusion | Cannot completely clear |
| Mixed with tissue | Extraction damages normal tissue |
| Often illegal injection | Very high risk |
⚠️ Warning: Silicone oil filler extraction is extremely difficult, usually can only improve rather than cure, and may require multiple surgeries. The best strategy is "prevention"—don't accept injections from unknown sources.
Why FILLER REVISION's Extraction Technique Succeeds Where Others Failed
Most filler lump extraction failures stem from one root cause: operating without real-time imaging. Without ultrasound guidance, the surgeon is essentially working blind — unable to distinguish filler boundaries from normal tissue, unable to track migrated material, and unable to confirm complete clearance. At FILLER REVISION, every extraction is performed under continuous high-resolution ultrasound navigation. This means we can trace filler deposits that have migrated far from their original injection site, separate material from tissue planes that appear fused to the naked eye, and verify in real time that nothing has been left behind. Combined with our sub-20% incision standard and material-specific extraction protocols, this approach consistently achieves thorough clearance in cases that other clinics deemed impossible.
How to Preserve Normal Tissue?
Technical Keys
← Swipe to see more →
| Technique | Explanation |
|---|---|
| Layer recognition | Understand anatomical layers, separate correctly |
| Blunt dissection | Use blunt instruments when possible, reduce bleeding |
| Conservative excision | Only remove confirmed foreign material |
| Intraoperative confirmation | Ultrasound real-time check for residue |
| Staged approach | Multiple sessions if needed to avoid excess damage |
Avoiding Over-Extraction
Over-extraction can cause:
- Tissue depression
- Functional impact (lips, nose)
- Unnatural appearance
- Need for secondary filling
💡 Dr. Liu's Philosophy: "I'd rather do two sessions than extract too much at once. Depression from over-extraction is harder to fix than the original lump."
Frequently Asked Questions
Can hyaluronic acid lumps be dissolved with hyaluronidase?
A1: It depends:
- Newly injected HA (Hyaluronic Acid) (< 1 year): Usually dissolvable
- Old or encapsulated: Hyaluronidase has limited effect, may need surgery
- Mixed with other fillers: Hyaluronidase only works on HA
Recommend trying dissolution first; consider surgery if ineffective.
Will minimally invasive extraction leave scars?
A2: Minimally invasive extraction pinholes are usually very small (1-2mm) and designed in concealed locations (hairline, inside nostril, inside mouth). Scars are virtually invisible and far better than leaving the lump untreated.
Will my face look sunken after extraction?
A3: With proper extraction, there won't be obvious depression. But if the original lump was large or in a special location, post-extraction may require:
- Waiting for tissue recovery (3-6 months)
- Modest filling (using safe hyaluronic acid)
Is general anesthesia needed?
A4: Most cases require only local anesthesia. Only consider gentle pain-relief anesthesia for very large areas, very deep locations, or multiple sites needing treatment.
Will the lump grow back after minimally invasive extraction?
A5:
← Swipe to see more →
| Filler Type | Recurrence Risk |
|---|---|
| Hyaluronic Acid | Very low (won't recur if completely removed) |
| Radiesse | Low (Liusmed minimally invasive technique ensures complete removal) |
| Collagen Stimulator | Low (Liusmed minimally invasive technique ensures complete removal) |
| Ellansé | Low (Liusmed minimally invasive technique ensures complete removal) |
| Silicone | High (often cannot completely clear, but can significantly reduce silicone residue) |
Collagen stimulator lumps require particularly close follow-up.
Post-Op Recovery and Follow-Up
Post-Op Timeline
← Swipe to see more →
| Period | Status and Care |
|---|---|
| Days 1-3 | Swelling peak, ice to reduce swelling |
| Week 1 | Swelling subsiding, return for evaluation |
| Week 2 | Suture removal (if applicable) |
| Month 1 | Tissue recovering |
| Month 3 | Evaluate final result |
| 6-12 months | Long-term follow-up (especially for collagen stimulator) |
Guidelines
← Swipe to see more →
| ✅ OK | ❌ Avoid |
|---|---|
| Ice to reduce swelling | Heat (first 3 days) |
| Normal diet | Irritating foods |
| Light activity | Strenuous exercise (2 weeks) |
| Attend follow-ups | Self-treating problems |
Conclusion: FILLER REVISION's Approach to Filler Lump Extraction
← Swipe to see more →
| Key Point | Explanation |
|---|---|
| Core principles | Precise localization, conservative excision, confirm completeness |
| Technical support | Ultrasound guidance greatly improves precision |
| Material differences | Different fillers need different strategies |
| Prevention is best | Choose reputable clinics, legitimate fillers |
At FILLER REVISION, we have built our practice around solving the cases other clinics cannot. If you have a filler lump that has resisted previous treatment attempts — or if you have been told your primary option is open surgery — we invite you to see what ultrasound-guided precision extraction can achieve.
Related Reading
- When Can Failed Aesthetics Be Repaired? Ultrasound-Guided Evaluation
- Multi-Layer Filler Extraction: Clearing Deposits Single-Approach Methods Miss
- Safe Filler Extraction Near Facial Nerves and Vessels
- Told You Need Surgery for Filler Lumps? Scar-Free Alternatives
- Blind Extraction Made It Worse? How to Repair the Damage
- Forehead and Temple Filler Extraction: High-Risk Zone Safety
- Under-Eye Filler Extraction: The Face's Most Delicate Zone
About the Author
Dr. Ta-Ju Liu
- Current Position: Director, Liushi Clinic
- Specialties: Minimal incision surgery (lipoma, cyst), hyperhidrosis surgery, thread lifting
- Experience:
- 15+ years of clinical minimal incision surgery experience
- Over 10,000 successful minimal incision cases
- Board-certified dermatologist
- Philosophy: "Filler lump treatment requires precision and patience. My goal is to remove the problem while preserving the patient's natural appearance."