
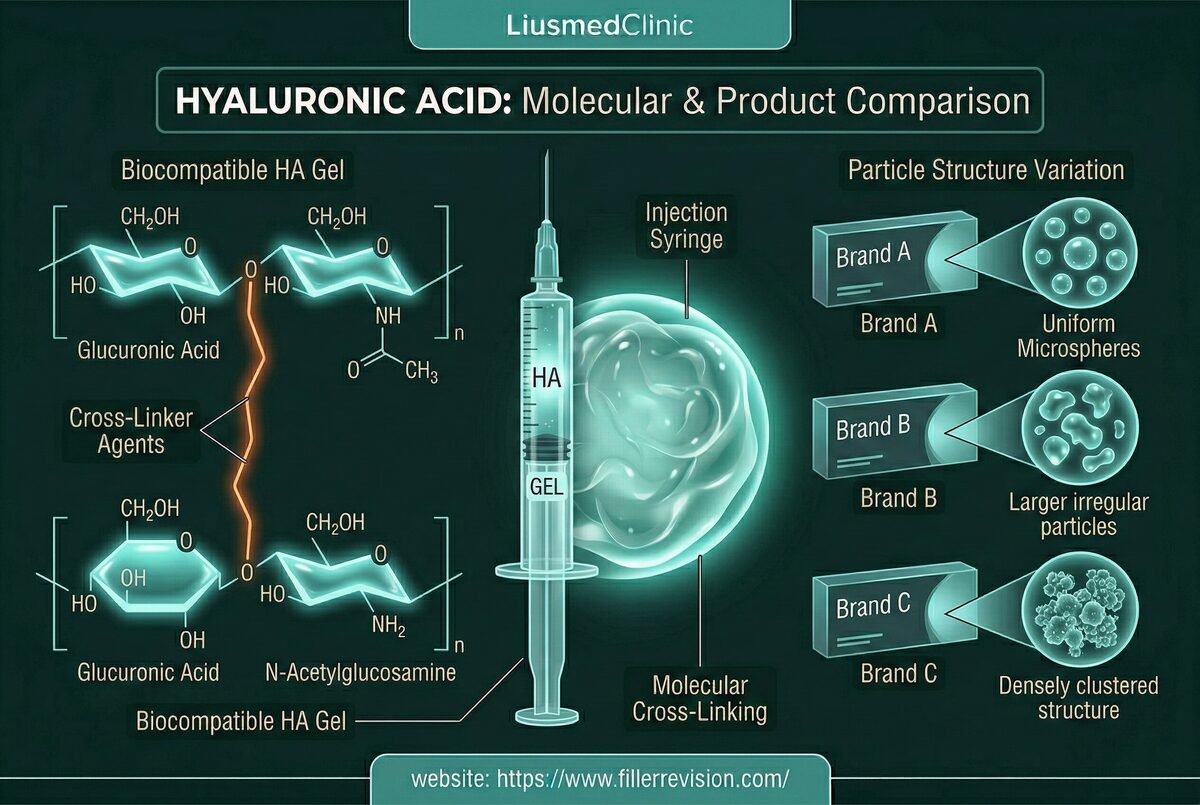
Hyaluronic Acid (HA) Complications
"I've had hyaluronidase three times now — the lump goes down a little, then comes right back. My injector says there's nothing left, but I can feel it." If this sounds like your experience, you're not imagining things. At FILLER REVISION, most of the HA patients we treat have already been through 2-3 failed dissolution attempts before finding us. Migration, encapsulation, chronic edema, and the Tyndall effect (bluish tint) can persist for years despite multiple dissolution attempts. Studies show that HA filler can remain detectable on ultrasound up to 10 years post-injection, particularly when encapsulated by fibrotic tissue. What your previous doctor likely didn't explain: once a fibrous capsule forms around the filler, enzymes physically cannot reach it — no matter how many times they inject.
Common Symptoms
The Mechanics of HA Complications
You didn't do anything wrong by trying dissolution first — it's the standard treatment and it works when the filler is accessible. But when you've been through multiple rounds and the lump persists, something else is going on. Repeated injections in the same area create layered deposits that compress and displace tissue planes. Over time, muscle movement pushes product into pockets of least resistance—explaining migration patterns from lips to the perioral shelf or from tear troughs to the malar region. Low-cohesivity products are particularly prone to spreading. When HA persists beyond its expected lifespan, the body mounts a foreign body response, forming a fibrous capsule around the deposit. This encapsulation effectively shields the filler from enzymatic dissolution, creating the frustrating clinical scenario where hyaluronidase injections produce no visible improvement.
Why Traditional Treatments Fail
Limitations of Enzyme Dissolution
Hyaluronidase is the standard treatment for HA complications, but its efficacy drops dramatically when the filler is encapsulated. The enzyme cannot penetrate the dense fibrous capsule wall, leaving the core filler intact. Blind injection of hyaluronidase also risks dissolving the patient's own native hyaluronic acid in surrounding tissue, causing volume loss and tissue hollowing in unintended areas. Repeated high-dose enzyme treatments can trigger allergic sensitization. Furthermore, without imaging guidance, clinicians cannot verify whether the filler has actually been dissolved or simply compressed to a different plane—leading to multiple ineffective treatment cycles.
“When a patient tells me they've had hyaluronidase three times and the lump is still there, I already know what the ultrasound will show: a bright capsule wall surrounding the filler, completely intact. Their previous doctors weren't wrong to try dissolution — they just didn't have the imaging to see that the filler had become unreachable. At FILLER REVISION, we see this every week. The moment the capsule appears on screen, the patient finally understands why nothing worked before.”
Dr. LiuWhy 'Just Dissolve It' Often Fails
Ultrasound-Guided Pinhole Micro-Extraction
Long-standing HA filler develops fibrous capsules that physically block enzyme from reaching the product inside. The single most important diagnostic question is whether a deposit is encapsulated or free-flowing — because this distinction alone determines whether enzyme injection will work or whether a completely different dual-mechanism approach is needed.
The Reason 2-3 Rounds of Dissolving Failed You
At FILLER REVISION, we see this pattern every week: a patient has had multiple rounds of hyaluronidase elsewhere with no lasting result. The reason is always the same — a fibrous capsule has formed around the filler, creating a physical wall the enzyme cannot penetrate.
One Ultrasound Scan Answers the Question Others Couldn't
Your previous clinic treated you without seeing inside. Encapsulated and free-flowing HA look identical from the outside but require completely different approaches. The scan that should have been done before your first dissolution attempt reveals exactly why nothing worked.
Verified Removal — Not Another 'Let's Try Again'
We don't dissolve and hope. We image, identify, and extract — then verify clearance on ultrasound before you leave. Most patients who've been through the dissolve-and-pray cycle elsewhere are done in a single session at FILLER REVISION.
Ultrasound-Guided Targeted Removal
We use high-frequency ultrasound to visualize every filler deposit in real time, identifying encapsulated versus free-flowing product. For encapsulated HA, we first perform capsulotomy—mechanically disrupting the fibrous wall—before delivering enzyme directly into the exposed core. For product that has migrated or formed deep deposits, we use direct needle aspiration under ultrasound guidance. This dual physical-plus-biochemical approach resolves cases that pure enzymatic dissolution cannot, achieving near-complete clearance in a single session.
Ultrasound Mapping
Capsule Disruption
Targeted Dissolving/Aspiration
Compression & Verification
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
The vast majority can be removed or significantly reduced in a single session. Ultrasound allows us to verify clearance in real time, so we know exactly how much remains. Encapsulated deposits that resist enzyme dissolution are treated with capsulotomy first, then enzyme or aspiration. Success rates exceed 95% when combining ultrasound guidance with physical removal techniques.
Skin has natural elasticity and typically retracts well after filler removal. The risk of visible sagging is mainly a concern when very large volumes have been in place for years, significantly stretching the skin. In most cases, patients are pleasantly surprised by how natural they look. For high-volume removals, we can discuss skin tightening protocols as a secondary step.
When HA filler persists in tissue for an extended period, the body forms a fibrous capsule around it—essentially a scar tissue shell. Hyaluronidase cannot penetrate this wall to reach the filler core. This is why repeated enzyme injections fail. The solution is to first disrupt the capsule under ultrasound guidance, exposing the filler to the enzyme, or to physically aspirate the encapsulated material directly.
A typical session takes 30-60 minutes depending on the number of areas and complexity. Most patients need only one session. Complex cases with multiple encapsulated deposits or extensive migration may require a follow-up session 2-4 weeks later to address residual product identified on ultrasound.
Yes, once healing is complete (usually 2-4 weeks), you can have fresh filler placed. Many patients choose to restart with a more conservative approach, using higher-cohesivity products and smaller volumes. We provide ultrasound verification before re-injection to confirm the area is clear.
Encapsulated HA appears as a well-defined, hyperechoic (bright) mass with a distinct surrounding capsule wall visible as a dark rim. Free-flowing or recently injected HA appears as an anechoic (dark) pool without defined borders. This distinction is critical because it determines whether enzyme alone will work or whether capsulotomy is needed first.
This is the most common scenario we treat. When multiple dissolution attempts fail, it almost always means the filler has become encapsulated — surrounded by a fibrous scar capsule that physically blocks the enzyme from reaching the filler inside. No amount of additional enzyme will penetrate this wall. The solution is ultrasound-guided capsulotomy: physically disrupting the capsule wall first, then applying enzyme directly to the exposed core, or aspirating the material entirely.
Ultrasound definitively answers this question. HA filler has a characteristic appearance on ultrasound that is clearly distinguishable from scar tissue, fat, or other structures. In our experience, patients told they have 'just scar tissue' frequently turn out to have encapsulated filler that is very treatable. Ultrasound imaging removes the guesswork and shows exactly what's inside.
The procedure is performed under local anesthesia. Most patients report only mild pressure sensation during the extraction. The ultrasound probe itself is painless. Post-procedure discomfort is minimal—mild swelling and tenderness for 2-3 days, manageable with standard over-the-counter pain relief.
Because we're not doing the same thing again and hoping for a different result. If dissolution failed, your filler is almost certainly encapsulated — surrounded by a fibrous wall that blocks the enzyme. We first identify the capsule on ultrasound, then physically disrupt it before applying enzyme to the exposed core, or aspirate the material directly. It's a fundamentally different mechanism, not a repeat attempt.
You are. Without ultrasound, there's no way to confirm whether filler has actually been removed or merely compressed. We regularly see patients told 'it's all gone' whose ultrasound reveals significant encapsulated deposits. The imaging doesn't lie — if you can feel it, it's worth scanning.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Duranti F, et al. Injectable hyaluronic acid gel for soft tissue augmentation. A clinical and histological study. Dermatol Surg. 1998;24(12):1317-1325.
- Requena L, et al. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1-34.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.