Three months after a Sculptra treatment, a patient notices a firm nodule on the cheek. Six months later, after five rounds of steroid injections, the lump still hasn't resolved — and ultrasound reveals a dense fibrous capsule encasing the poly-L-lactic acid (PLLA) particles. This scenario is not rare: delayed-onset nodules (DON) occur in an estimated 3–5% of Sculptra cases in some series, and a subset progress to true foreign body granulomas that show high resistance to pharmacological treatment.
This guide is for patients who have developed a hard lump, nodule, or granuloma after Sculptra, or who have been told their complication may be a granuloma. Understanding each step — from correctly identifying the nodule type, to knowing when steroid therapy is no longer the right tool — can prevent years of unsuccessful treatments.
For a broader overview of collagen-stimulator (PLLA / PCL / CaHA) complications, see the Collagen Stimulator Conditions Overview.
What to Do About a Sculptra Hard Lump: The First Assessment Steps
A firm spot that can be felt but not seen after a Sculptra injection does not automatically indicate a problem. The biological mechanism of PLLA — sustained low-grade controlled inflammation that stimulates collagen — means some degree of early firmness is expected. The following table helps classify which category a lump falls into:
← Swipe to see more →
| Type | Onset | Characteristics | Recommended Action |
|---|---|---|---|
| Normal swelling | Days 0–7 | Diffuse swelling, no focal hard point, non-tender | Observe, gentle massage |
| Early small nodules | Weeks 1–4 | Palpable but invisible micro-particles, scattered | Active massage, re-assess at 4–6 weeks |
| Delayed onset nodule (DON) | Week 4 to years later | Single or few firm, discrete nodules; may be visible | Specialist assessment required |
| True granuloma | Usually > 3 months | Hard, fixed, encapsulated, possibly tender | Active intervention needed |
| Infection / biofilm | Any time | Redness, warmth, swelling, purulence, significant tenderness | Seek immediate medical care |
More than half of small nodules that appear within the first three months resolve spontaneously with consistent massage. There is no need to panic. However, specialist assessment is appropriate if any of the following apply:
- The lump has not decreased in six or more months
- A visible surface elevation or asymmetry is present
- Tenderness is present and worsening over time
- Steroid injection provided temporary improvement followed by recurrence
Key point: "Palpable but invisible" does not equal urgent. The relevant question is whether the lump is shrinking, stable, or growing — and whether it is causing discomfort or visible change. Accurate classification prevents unnecessary early interventions and also prevents the opposite: waiting too long when true encapsulation has already begun.
Can Sculptra Nodules Be Removed? A Full Comparison of Non-Surgical and Surgical Options
The direct answer: Sculptra nodules can be treated, but the concept of "removal" is fundamentally different from that of hyaluronic acid (HA) fillers.
HA filler is a cohesive gel that can be dissolved by hyaluronidase (a dissolving enzyme) with high precision. Sculptra, by contrast, is a microparticle suspension — tens of thousands of PLLA particles dispersed throughout the tissue. There is no enzymatic agent that dissolves PLLA, and the dispersed nature of the particles makes "extraction of the whole mass" impossible in most cases. The four clinical options available are:
Option A: Intralesional Corticosteroid Injection (Triamcinolone Acetonide)
Mechanism: Direct injection of triamcinolone (Kenalog) into the nodule suppresses immune-mediated inflammation and reduces aberrant collagen deposition.
Appropriate when: The nodule is still in the inflammatory phase (tender, mildly red), has been present less than six months, and capsule formation is minimal.
Limitations: Once significant fibrous encapsulation has occurred, the capsule acts as a barrier that prevents adequate steroid penetration to the PLLA particle core. Repeated injection attempts with no sustained improvement are a strong clinical signal that encapsulation is the underlying problem.
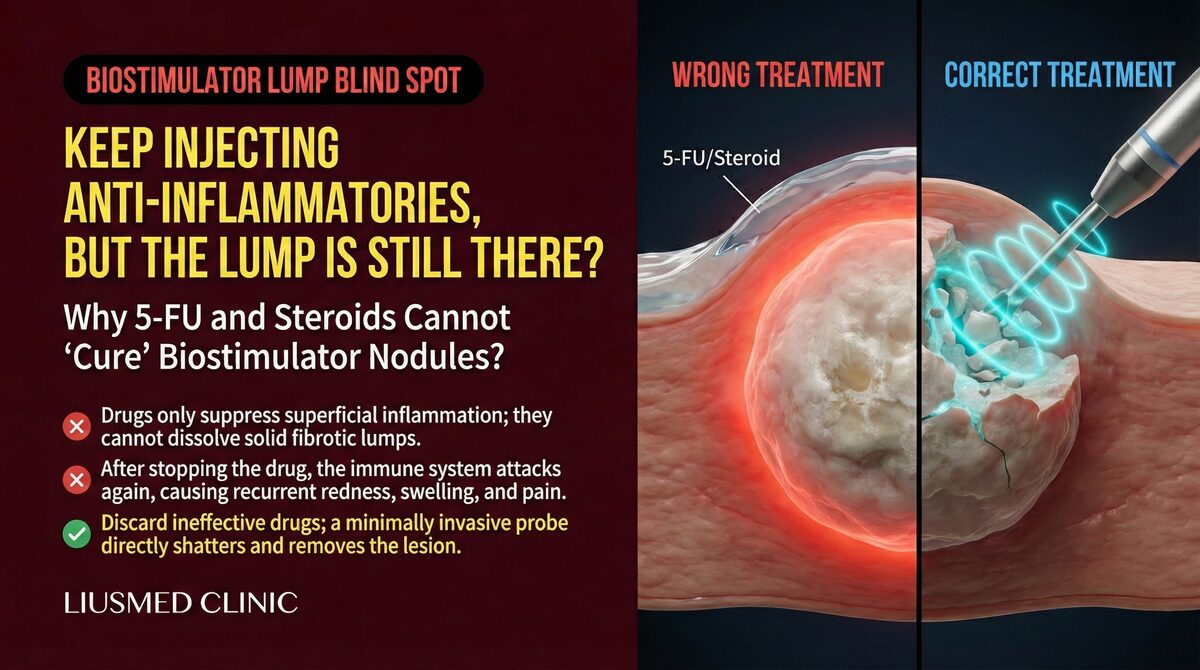
Option B: 5-Fluorouracil (5-FU) Combined with Corticosteroid
5-FU is an antineoplastic agent with anti-fibrotic properties in dermatological use, targeting the fibrous component of granulomas. In combination with steroids — which address the inflammatory component — the theoretical basis is sound, and published case series report positive outcomes for early-stage PLLA nodules.
The practical limitation is the same penetration barrier. For heavily encapsulated chronic PLLA granulomas, pharmacological agents continue to underperform regardless of the combination used.
For a detailed analysis of why 5-FU fails in encapsulated collagen-stimulator nodules, see: The Limitations of 5-FU for Collagen Stimulator Lumps
Option C: Ultrasound-Guided Physical Extraction
Under real-time high-frequency ultrasound guidance, a micro-cannula or aspiration instrument is advanced through a single 1–2 mm access point, directly targeting the encapsulated PLLA nodule. The capsule is mechanically disrupted and the loosened PLLA particles and fibrous tissue are aspirated.
The core principle is "see it before you treat it" — ultrasound imaging allows the physician to identify nodule size, depth, and proximity to critical structures before any instrument enters the tissue, rather than working blindly.
Best suited for: Cases where steroids and/or 5-FU have failed at least twice; clinical or ultrasound evidence of significant encapsulation; a single large, isolated, well-defined nodule; or patients who require a more definitive resolution.
Realistic expectations: In most cases, a significant reduction in nodule volume and resolution of visible surface irregularity can be achieved. Claims of "100% complete removal of all PLLA particles" are not clinically supportable — the microparticle nature of PLLA means total clearance confirmed on imaging has not been established in the literature. The goal is functional and aesthetic resolution, not a theoretically perfect scan.
Option D: Open Surgical Excision
For anatomically localized confirmed granulomas — particularly in specialized areas such as the periorbital region — open excision remains a valid option. The primary tradeoff is the risk of visible scarring at the excision site. With advances in minimally invasive techniques, surgical excision is less commonly used as a first-line approach.
Key point: These options are not mutually exclusive. Early inflammatory nodules can reasonably begin with steroids. When encapsulation is established and drugs have repeatedly failed, continuing the same pharmacological approach produces diminishing returns, and minimally invasive removal is often the more reliable next step. Correct staging of the nodule — inflammatory versus fibrotic, encapsulated versus non-encapsulated — is the decision tree's starting point.
Sculptra Delayed Onset Nodules (DON): Why They Appear Months Later
"Why did my nodule only appear six months after the injection?" is a common clinical question. The answer lies in the distinct mechanism of delayed onset nodules (DON) compared with early technical nodules.
Early Nodule vs. DON: Two Different Problems
← Swipe to see more →
| Early Nodule (< 4 weeks) | Delayed Onset Nodule DON (> 4 weeks) | |
|---|---|---|
| Cause | Technical: uneven dilution, superficial injection, inadequate massage | Immunological: T-cell–mediated delayed-type hypersensitivity (Type IV) |
| Histopathology | Local PLLA particle aggregation | Foreign body granuloma — macrophages, epithelioid cells, multinucleated giant cells (MGC) surrounding PLLA particles |
| Texture | Small, scattered, may resolve spontaneously | Firm, fixed, discrete, single or few |
| Treatment response | Massage and observation usually effective | Variable pharmacological response; high failure rate after encapsulation |
The immunological mechanism of DON: PLLA particles degrade slowly over 2–5 years, continuously releasing antigenic signals during that period. In susceptible individuals, this sustained antigenic stimulus triggers a delayed-type hypersensitivity (DTH) response — immune cells cluster around PLLA particles and form granulomatous inflammation, inducing fibroblast proliferation and collagen deposition that progressively hardens into a fibrous capsule.
Reported triggers: Published case reports document a temporal association between systemic immune activation (viral illness, vaccination) and the onset of previously quiescent DON. This does not mean vaccination causes DON; rather, tissue containing dormant PLLA particles may develop focal immunological activity when the systemic immune system is broadly activated.
Why DON is particularly treatment-resistant: Once a fibrous capsule forms, it simultaneously blocks drug penetration to the PLLA core and shields the particles from phagocytic clearance — creating a pharmacological standstill where standard treatment agents cannot reach their target.
PLLA Granuloma Risk Factors: Not Random, and Traceable
With thousands of successful Sculptra treatments worldwide, why do granulomas occur in some patients and not others? Identifiable risk factors exist on both the technical and patient-specific side.
Injection Technique Factors
1. Superficial injection depth PLLA should be deposited in the subcutaneous fat or supraperiosteal plane. Intradermal or superficial subdermal injection places PLLA particles in a microenvironment with high immune cell density and poor vascular supply, significantly increasing granuloma incidence.
2. Insufficient dilution Current guidelines recommend diluting one vial of Sculptra in ≥ 7–9 mL of sterile water. Earlier protocols using only 3–5 mL produced higher particle concentrations in tissue. Many legacy cases of PLLA granuloma — including cases presenting years after injection — trace back to the older dilution regimen.
3. Inadequate post-injection massage The "5-5-5 massage rule" (5 minutes, 5 times daily, 5 days post-injection) is designed to distribute PLLA particles evenly and prevent focal aggregation. Insufficient massage creates locally concentrated particle clusters that increase granuloma trigger probability.
4. Excessive injection volume per session Particularly in the deep zygomatic region, high single-session volumes increase regional granuloma risk regardless of other technical factors.
Patient-Specific Factors
- Autoimmune predisposition: Patients with a history of Sjögren's syndrome, systemic lupus erythematosus, or rheumatoid arthritis have a higher baseline risk of PLLA-induced granuloma and should receive detailed pre-procedure counseling.
- Pre-existing biofilm: Areas with a history of prior filler injections may harbor subclinical biofilm. PLLA injection into these areas can precipitate infection-triggered granuloma — a distinct subtype requiring antibiotic biofilm treatment before the nodule can be adequately reduced.
- Thin skin and minimal subcutaneous fat: Periorbital and neck regions have less fat buffer between skin and any injected PLLA, placing particles closer to the dermis where immune activity is higher.
Key point: PLLA granuloma formation is rarely fully random. In most cases, one or more identifiable risk factors can be traced retrospectively. This is an argument for thorough pre-procedure assessment — immune history, prior filler history, tissue thickness — rather than treating Sculptra as a universally "low-risk" collagen stimulator.
For further reading on 5-FU treatment limitations in collagen-stimulator granuloma: Collagen Stimulator Lumps and 5-FU Treatment Failure
After Steroid and 5-FU Failure: Advanced Revision Strategies
For context on why repeated steroids fail to resolve encapsulated PLLA nodules, see: Why Sculptra Lumps Don't Respond to Repeated Steroid Injections
The most common clinical path for unresolved Sculptra nodules is: initial steroid injection → partial temporary improvement → recurrence → second steroid injection → diminishing response. If this cycle has repeated twice or more, continuing the same approach is unlikely to produce a different outcome. The strategic reframe at this point is: assess the nodule's actual anatomical and biological state, then choose a tool that matches it.
Step 1: Ultrasound Assessment of Encapsulation
High-frequency ultrasound (15–22 MHz) is the key evaluation tool before any further intervention. An encapsulated PLLA granuloma presents with:
- A hyperechoic, densely structured capsule border
- Internal echogenic foci representing PLLA particle aggregates
- Increased perinodular blood flow on Doppler, indicating active inflammation
Clinical interpretation: When capsule thickness exceeds approximately 1 mm and nodule diameter exceeds 8 mm, drug penetration through the capsule is substantially reduced. At this stage, physical disruption of the capsule structure typically yields more reliable results than additional injection attempts.
Step 2: Ultrasound-Guided Mechanical Capsule Disruption and Aspiration
Under real-time ultrasound guidance:
- Fine-needle entry into the capsule, with a small volume of saline or steroid solution to soften the capsule interior
- Micro-cannula insertion through a single 1–2 mm access point to mechanically disrupt the capsule structure
- Negative-pressure aspiration of fragmented PLLA particles and fibrous tissue
- Real-time ultrasound verification of residual volume
In most cases, this achieves substantial reduction of residual nodule volume and resolution of visible surface irregularity. As noted earlier, confirmed total clearance on imaging is not a realistic endpoint given the microparticle nature of PLLA — the clinical goal is relief of symptoms and aesthetic improvement.
Step 3: Post-Procedure Management and Follow-Up
- Week 1: Antibiotic coverage if any signs of infection or biofilm are present
- Months 3–6: Ultrasound follow-up to assess residual PLLA signal and local inflammatory activity
- If symptomatic residual nodule persists: evaluate need for second-session intervention
Emerging Options (Evidence Still Accumulating)
JAK inhibitors: There is accumulating clinical evidence that JAK inhibitors (targeting the JAK-STAT immune signaling pathway) can provide partial improvement in injection-related granulomas unresponsive to conventional treatment. Standardized protocols are still being established; Dr. Liu will discuss this option based on each patient's individual case and current literature.
Frequently Asked Questions
Will treating the granuloma reverse Sculptra's collagen-stimulating effect?
Treating a granuloma does not undo Sculptra's cosmetic benefit. A granuloma represents pathological over-fibrosis, not the desired controlled collagen induction — removing it addresses the problem tissue, not the treatment result. In cases where granuloma involves the majority of the treated region, the overall aesthetic assessment should be discussed individually with the physician.
Can I ask to have all the Sculptra removed?
Because PLLA is a microparticle suspension rather than a cohesive mass, there is no "total extraction" equivalent to removing an HA filler. Symptomatic nodules and granulomas can be substantially cleared. Asymptomatic PLLA particles distributed in soft tissue do not require — and realistically cannot be — completely removed. The assessment focus should be on whether a specific symptom or visible concern is causing distress, not on achieving zero residual PLLA.
The lump got smaller after steroid injection but came back. What does that mean?
This is the classic encapsulation pattern: steroids reduce perilesional inflammation and the nodule appears to shrink transiently, but the drug has not penetrated the capsule to address the PLLA core. When inflammation restarts, the nodule rebounds. The cycle of partial shrinkage and recurrence is a clinical indicator that the current treatment modality is insufficient and escalation should be considered.
Does every delayed onset nodule need treatment?
Not necessarily. If a nodule can be felt but not seen, causes no discomfort, and shows no progression, observation may be appropriate — some DON cases resolve as PLLA gradually degrades over several years. Active intervention is indicated when there is visible surface elevation, progressive enlargement, significant tenderness, or failure to respond to pharmacological treatment.
If your Sculptra nodule has been present for more than six months and has not responded to two or more rounds of steroid treatment, waiting further is rarely in your interest — the longer encapsulation persists, the more challenging any subsequent intervention becomes.
Dr. Ta-Ju Liu uses ultrasound-guided minimally invasive techniques and has managed multiple cases of treatment-resistant PLLA granuloma with significant encapsulation. Visit the Filler Revision Clinic service page to understand the full assessment and treatment process, then schedule a consultation to discuss your individual case.
Dr. Ta-Ju Liu | Filler Revision Clinic — fillerrevision.com