Why Won't My Sculptra Lumps Go Away After Steroid Injections?
"I've had four rounds of steroid injections for my Sculptra lumps. They get a little softer each time, but they always come back." At FILLER REVISION, this is one of the most common stories we hear. Patients arrive frustrated after months or years of repeated pharmacological treatments that never fully resolve the problem. In our clinical experience, the vast majority of Sculptra nodule patients who reach us have already attempted steroids, 5-FU (5-Fluorouracil), or both — and the lumps persist. Steroid and 5-FU treatments have a ceiling of effectiveness against encapsulated Sculptra nodules, and understanding why helps clarify what treatment can actually work.
Understanding Sculptra and Why Nodules Form
What Is Sculptra?
Sculptra is an injectable containing poly-L-lactic acid (PLLA) microparticles suspended in a water-based solution. Unlike hyaluronic acid fillers that provide immediate volume, Sculptra works by stimulating the body to produce its own collagen over several months.
← Swipe to see more →
| Characteristic | Detail |
|---|---|
| Active ingredient | Poly-L-lactic acid (PLLA) |
| Mechanism | Collagen stimulation, not direct filling |
| Duration | 2–3 years or longer |
| Dissolvable | No enzyme or medication available |
| FDA (U.S. Food and Drug Administration)-approved uses | Facial volume restoration, HIV lipoatrophy |
Why Do Sculptra Nodules Form?
Nodule formation with Sculptra occurs through several mechanisms:
← Swipe to see more →
| Cause | Mechanism |
|---|---|
| Insufficient dilution | Concentrated PLLA (Poly-L-Lactic Acid) particles cluster and provoke stronger tissue reaction |
| Inadequate massage | Uneven distribution creates focal areas of high PLLA concentration |
| Wrong injection plane | Superficial placement in areas with thin tissue coverage |
| Patient susceptibility | Individual variation in foreign body response |
| High-risk areas | Periorbital region, lips, nose—areas with thin skin and limited tissue |
The Encapsulation Process
When PLLA particles concentrate in one area, the body responds with a foreign body granulomatous reaction:
- Macrophages surround the PLLA particles
- Giant cells form to engulf the foreign material
- Fibroblasts deposit collagen around the inflammatory focus
- A fibrous capsule forms, walling off the material
- The encapsulated nodule becomes a self-contained structure
Once this capsule is fully formed, the PLLA particles inside are effectively shielded from external treatments.
Key Insight: At FILLER REVISION, we see this pattern regularly — encapsulation is the body's defense mechanism against foreign material. Once complete, the capsule wall acts as a barrier that prevents medications—including steroids—from reaching the PLLA particles inside. This is why patients who have tried multiple steroid rounds without resolution need a fundamentally different approach.
Why Steroids and 5-FU Reach Their Limits
How Steroids Work on Nodules
Intralesional corticosteroids (typically triamcinolone acetonide) work by:
- Suppressing the inflammatory response around the nodule
- Reducing collagen synthesis by fibroblasts
- Softening the fibrous tissue through anti-inflammatory action
Why Steroids Fail on Encapsulated Nodules
← Swipe to see more →
| Stage | Steroid Effectiveness |
|---|---|
| Early inflammatory nodule (< 6 months) | Moderate to good—can reduce active inflammation |
| Partially encapsulated (6–12 months) | Limited—capsule restricts drug penetration |
| Fully encapsulated (> 12 months) | Poor—steroid cannot reach the PLLA core |
| Calcified or fibrotic (> 24 months) | Minimal—dense tissue blocks all penetration |
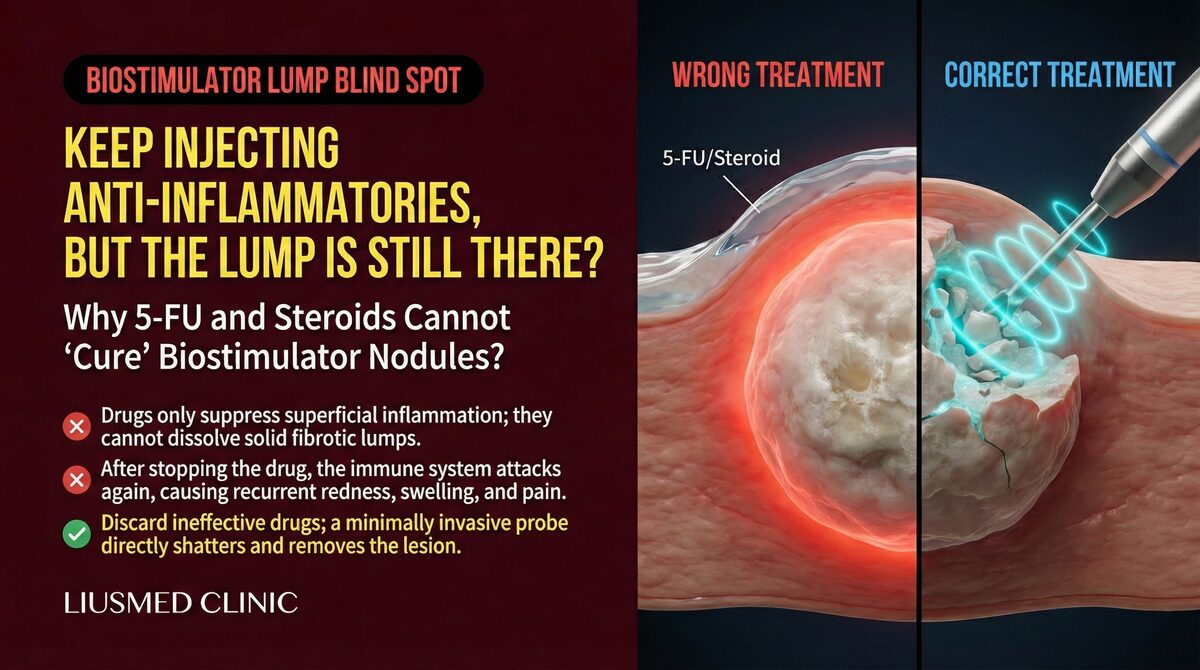
The fundamental problem: steroids work on the inflammatory component, but once encapsulation is complete, the primary issue is structural, not inflammatory. No amount of anti-inflammatory medication can dissolve a mature fibrous capsule.
The 5-FU Addition
5-Fluorouracil is sometimes combined with steroids in an attempt to inhibit fibroblast proliferation and reduce the fibrous capsule. While this can provide modest additional benefit in early nodules:
- Its penetration through mature capsules is limited
- It does not dissolve existing fibrous tissue
- Repeated injections carry risks of tissue damage
- Results are inconsistent for established nodules
Dr. Liu explains: "Steroids and 5-FU are reasonable first-line treatments for early Sculptra nodules. But if two or three rounds of injections have not significantly improved the lump, continuing the same approach is unlikely to yield different results. The capsule is simply too well-formed for medication to penetrate effectively."
The Risks of Repeated Steroid Injections
Tissue Atrophy: A Growing Concern
Each steroid injection carries cumulative risks that worsen with repetition:
← Swipe to see more →
| Complication | Description | Reversibility |
|---|---|---|
| Skin atrophy | Thinning of the skin overlying the nodule | Partially reversible over 6–12 months |
| Fat atrophy | Loss of subcutaneous fat around the injection site | Slowly reversible, may need filling |
| Telangiectasia | Visible dilated blood vessels on the skin surface | Often permanent |
| Hypopigmentation | Loss of skin color at the injection site | May improve but often persists |
| Dermal depression | Visible dip or crater around the nodule | May require secondary correction |
The Paradox of Over-Treatment
Repeated steroid injections can create a situation worse than the original nodule:
- The lump persists because the capsule is intact
- The surrounding tissue deteriorates from steroid effects
- The skin becomes thinner and more fragile
- Future extraction becomes more technically challenging due to compromised tissue quality
When Pharmacological Treatment Has Run Its Course: The FILLER REVISION Approach
The pattern we observe at FILLER REVISION is consistent: steroids and 5-FU work best on early, inflammatory Sculptra nodules — typically within the first six months. Beyond that window, the fibrous capsule matures and becomes a structural barrier, not an inflammatory one. Continuing steroid injections at this stage does not address the encapsulated PLLA core; instead, it risks progressive tissue atrophy and skin thinning that makes future correction more difficult. At FILLER REVISION, we recommend transitioning to extraction after two failed steroid rounds rather than persisting with diminishing returns. Our ultrasound-guided micro-extraction directly removes the capsule and its contents, achieving in one session what months of repeated injections could not accomplish.
The Definitive Solution: Ultrasound (Ultrasonography)-Guided Micro-Extraction
Why Physical Removal Works
When medications cannot penetrate the capsule, the logical solution is to bypass the capsule entirely through physical extraction. Ultrasound-guided micro-extraction:
- Directly accesses the encapsulated nodule through a pinhole incision
- Physically separates the capsule and PLLA material from surrounding tissue
- Removes the entire structure—capsule, PLLA particles, and granulomatous tissue
- Confirms completeness with real-time ultrasound verification
The Extraction Process
Pre-Operative Assessment:
- Detailed history: injection dates, volumes, areas, previous treatments
- Physical examination: palpation of all nodules, skin quality assessment
- Ultrasound mapping: location, depth, size, capsule characteristics, proximity to vital structures
The Procedure:
← Swipe to see more →
| Step | Detail |
|---|---|
| Anesthesia | Local anesthesia at and around the nodule |
| Incision | Pinhole entry point (1-2mm) in a concealed location |
| Approach | Ultrasound guides the instrument to the capsule |
| Separation | Careful blunt dissection separates the capsule from normal tissue |
| Extraction | The encapsulated material is removed through the pinhole |
| Verification | Ultrasound confirms adequate removal |
| Closure | Minimal or no sutures needed for the pinhole |
Post-Operative Care:
- Light pressure for 24 hours
- Ice application for the first 48 hours
- Avoid strenuous activity for 1 week
- Follow-up at 1 week, 1 month, and 3 months
What Makes This Different From Surgical Excision?
Traditional surgical excision involves a larger incision and wider tissue removal. Micro-extraction differs in several important ways:
← Swipe to see more →
| Factor | Traditional Excision | Micro-Extraction |
|---|---|---|
| Incision size | 5–15mm | 1-2mm |
| Tissue removal | Wider margins | Targeted capsule only |
| Scarring | Visible scar likely | Virtually invisible |
| Anesthesia | May need sedation | Local anesthesia |
| Recovery | 1–2 weeks | 3–5 days |
| Guidance | Visual or blind | Real-time ultrasound |
Recovery and Expected Outcomes
Post-Extraction Timeline
← Swipe to see more →
| Period | What to Expect |
|---|---|
| Day 1–3 | Mild swelling, possible bruising, manageable discomfort |
| Week 1 | Swelling resolving, follow-up assessment |
| Week 2–4 | Tissue remodeling, contour improvement |
| Month 1–3 | Progressive recovery, tissue softening |
| Month 3–6 | Final assessment, consider volume restoration if needed |
Managing Expectations
- Volume change: The area will appear flatter after nodule removal. This is normal and expected.
- Tissue quality: If multiple steroid injections were administered previously, the overlying skin may be thinner. Recovery of skin quality takes additional time.
- Secondary treatment: Volume restoration with safe HA (Hyaluronic Acid) filler is possible after 3–6 months of healing.
- Recurrence: Complete extraction has a very low recurrence rate. Follow-up ultrasound at 3 months confirms the outcome.
Dr. Liu's approach: "For patients who have been through multiple rounds of failed steroid treatment, I focus on two things: removing the nodule definitively, and assessing whether the surrounding tissue needs time or additional support to recover. The goal is not just lump removal but overall aesthetic restoration."
When Should You Stop Steroid Treatment and Consider Extraction?
Decision Framework
← Swipe to see more →
| Situation | Recommendation |
|---|---|
| First steroid injection, some improvement | Reasonable to try one more round |
| Two rounds with minimal change | Strongly consider extraction |
| Three or more rounds, lump persists | Stop steroids, proceed to extraction |
| Skin thinning or atrophy developing | Stop steroids immediately, assess for extraction |
| Multiple nodules in different areas | Comprehensive assessment with extraction planning |
The earlier you transition to extraction, the better the tissue quality and the easier the procedure.
Frequently Asked Questions
Can Sculptra nodules resolve on their own?
PLLA is biodegradable and eventually breaks down over 2–3 years. However, once a mature capsule has formed, the fibrous tissue itself does not resolve. Patients may notice some softening over years, but the nodule typically remains palpable.
Is the extraction procedure painful?
Under local anesthesia, most patients report only mild pressure during the procedure. Post-operative discomfort is minimal and manageable with standard pain relief.
What if I have nodules in multiple locations?
Multiple nodules can be addressed in a single session or staged over several appointments, depending on the number and location. A comprehensive ultrasound assessment determines the optimal approach.
Will the Sculptra I had still produce collagen after the nodule is removed?
The collagen that has already been produced by Sculptra in healthy areas remains intact. Extraction targets only the problematic nodules, not the normally distributed PLLA.
Move Beyond Repeated Failed Treatments
If you've already tried treatment for Sculptra nodules without success, FILLER REVISION specializes in exactly these cases. When steroids and 5-FU have reached their limits, our ultrasound-guided micro-extraction provides the definitive solution that pharmacological approaches cannot deliver.
About the Author
Dr. Ta-Ju Liu
- Current Position: Director, Liusmed Clinic
- Specialties: Minimally invasive surgery (lipoma, cyst), hyperhidrosis surgery, thread lifting, filler complication repair
- Experience:
- 15+ years of clinical minimally invasive surgery experience
- Over 10,000 successful minimally invasive cases
- Board-certified dermatologist
- Philosophy: "When medications have reached their limit, patients need a clear path forward—not more of the same treatment. Micro-extraction provides that definitive answer for encapsulated Sculptra nodules."