Key Facts:
- Patient: Woman in her 30s. Hyaluronic acid filler injected at another clinic into upper lip and nasolabial fold regions, developed vascular embolism signs.
- Delay: ~36 hours elapsed from embolism onset to FILLER REVISION referral — preceded by two days of high-dose extravascular hyaluronidase and hyperbaric oxygen at the original clinic, with continued skin deterioration.
- Rescue technique: Ultrasound-guided intra-arterial hyaluronidase injection (IAHA) — hyaluronidase delivered directly into the obstructed facial artery branch lumen, not flooded into surrounding tissue.
- Outcome: Full skin recovery at two weeks. No hyperpigmentation, no atrophic scarring; only mild residual numbness of the upper lip.
- Significance: Traditional teaching places the rescue golden window at 6-24 hours. This case succeeded at the rarely-documented 36-hour window, suggesting that the "ischemic penumbra" concept is clinically more resilient than previously assumed.
Could This Be Happening to Me Right Now?
If you've just received filler in the last 24-48 hours and are seeing changes that feel wrong, here's a rapid self-check:
- Skin in or near the injection area looks white, dusky purple, or has net-like (lacy) red-purple mottling — different from normal solid-color bruising
- Pain is disproportionate — sharper, deeper, or more persistent than typical post-injection soreness; described as burning or electric
- Any vision change, eye pain, blurring, or visual field defect — this is the most catastrophic sign and demands immediate emergency care
If you said yes to any of these: Contact your injector right now. If you cannot reach them within 10 minutes, go to the emergency room and say "I think I have a filler vascular occlusion." Bring the product box and lot number if possible. Photograph the area every 15 minutes en route. Do not ice, do not massage, do not "wait and see."
Why this matters: This 36-hour case succeeded because the patient acted at 36 hours rather than 48 or 72. The penumbra shrinks every hour — even one hour of delay can be the difference between full recovery and permanent scarring.
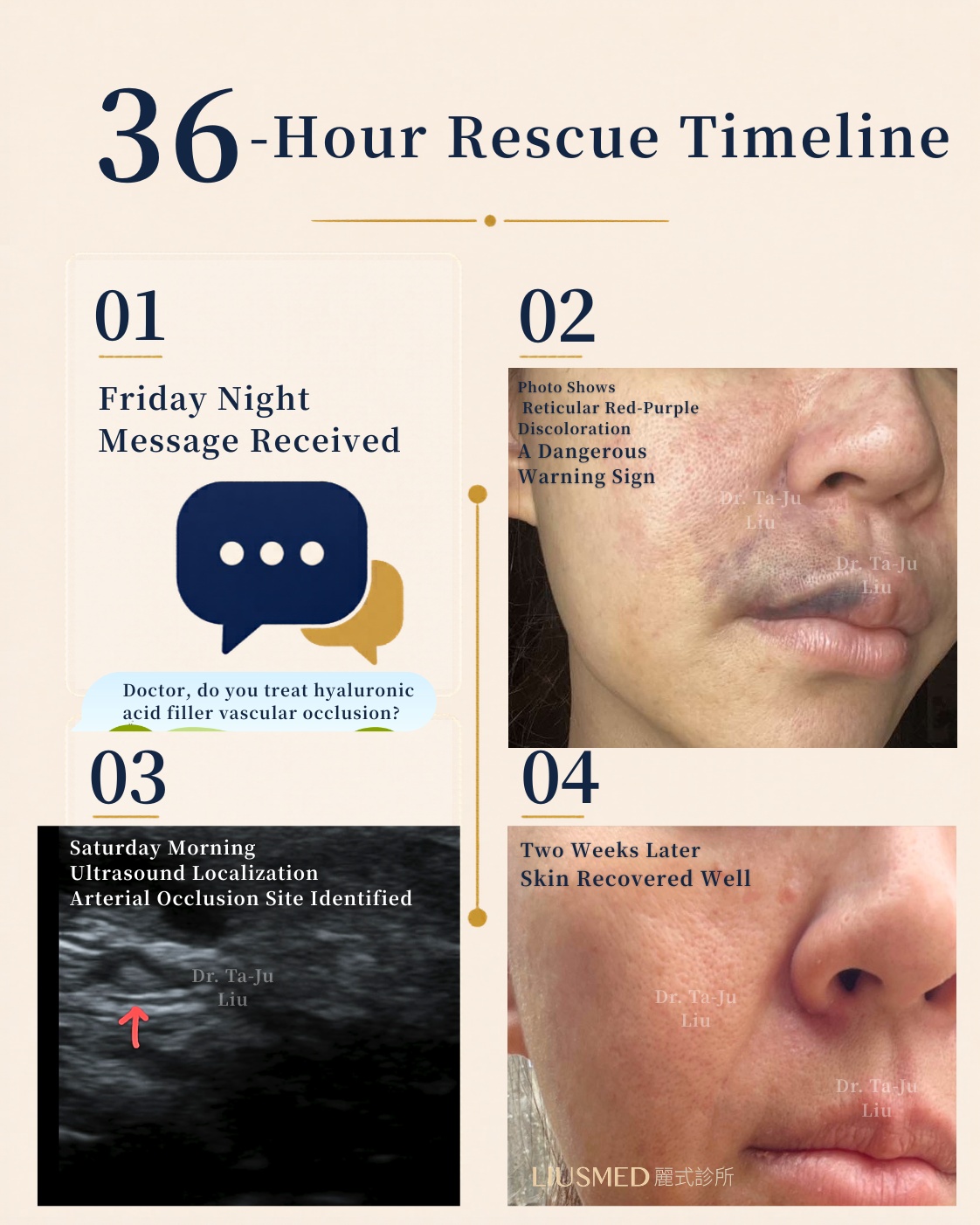
The Beginning of the Story: A Friday Night Message at 8 PM
One Friday evening, a message popped up on the FILLER REVISION Facebook page. I happened to see it:
"May I ask — can you treat hyaluronic acid embolism? 😭"
That sentence hit me. This was an emergency, so I opened the chat immediately and asked:
"How long since the embolism? What's the current situation? This is urgent — please send a photo of the affected area."
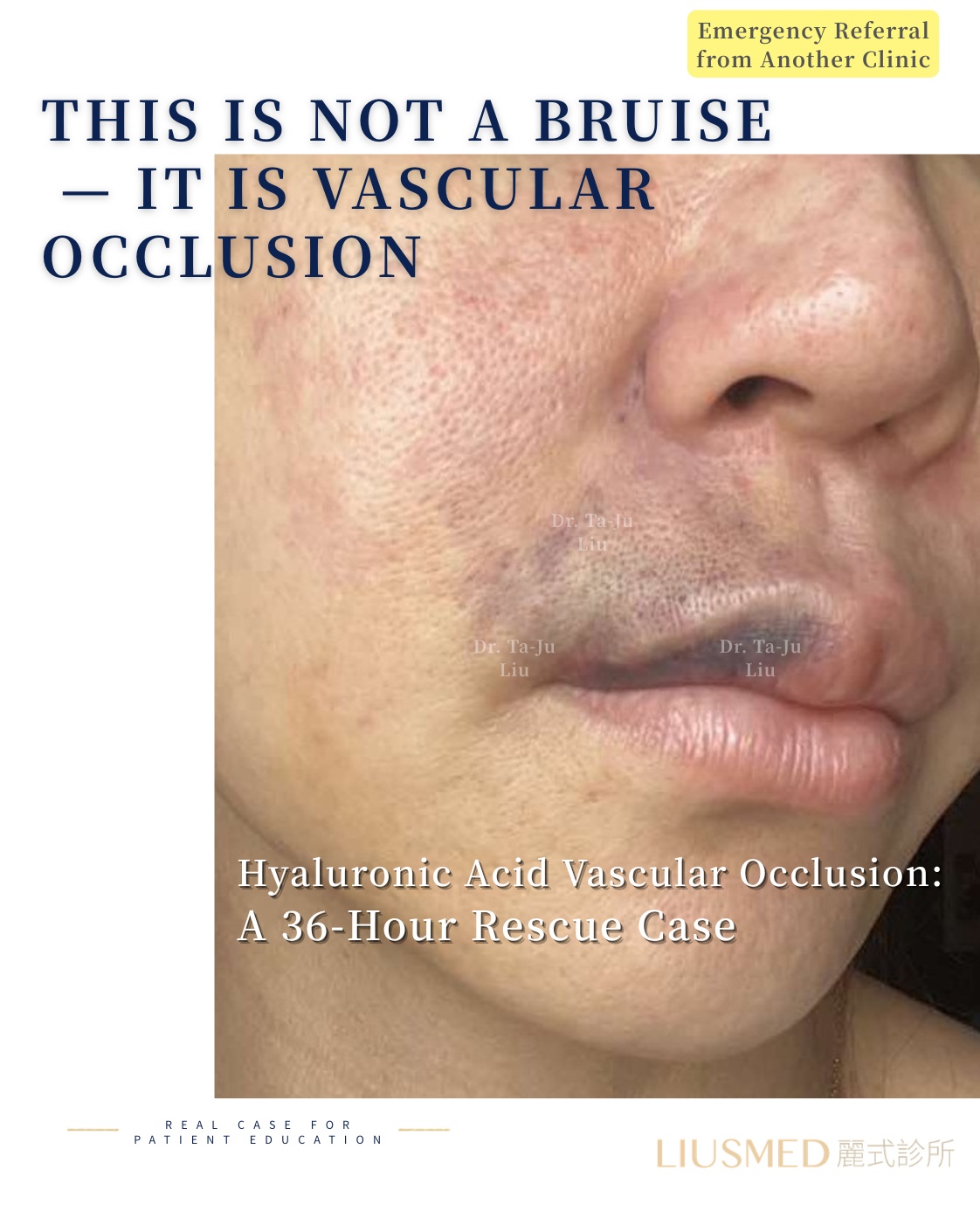
The photo came through: the right upper lip and nasolabial fold area showed a patch of net-like red-purple mottling.
That color and distribution were different from ordinary bruising. I knew at a glance: this was skin ischemia — vascular embolism. This characteristic livedo reticularis (a mottled, net-like bluish-purple skin pattern signaling impaired arterial blood flow — the textbook earliest sign, but the one most often mistaken for a regular bruise) is the most classic and most frequently missed warning sign.
I asked about her vision next — because once facial filler causes a vascular blockage, the worst-case scenario is not just skin necrosis. In rare cases, embolic material can travel via the terminal facial artery branches (the superior labial, lateral nasal, and angular arteries — the angular artery anastomoses with the dorsal nasal artery, which connects to the ophthalmic artery) and retrograde-embolize to the retinal artery, causing blindness.
Fortunately, her vision was unaffected.
I asked her to come in immediately. But it was already near the end of clinic hours, and she lived in Taichung — the last high-speed rail of the Friday evening had already left.
The 36-Hour Timeline
I worked through the details with her. The injection at the other clinic had targeted her upper lip and nasolabial fold. Right after the injection, she had immediate extensive bruising, swelling, pain, and numbness — these three together are already a high-suspicion sign for embolism. By the second day, small pustules had appeared near the nose along the nasolabial fold.
She had spent the two preceding days at the original clinic receiving high-dose extravascular hyaluronidase flooding and hyperbaric oxygen therapy (HBOT, breathing pure oxygen at 2.0-2.5 ATA to push more dissolved oxygen into ischemic tissue). But the red-purple mottled changes and the skin deterioration kept worsening.
By the time she reached FILLER REVISION, a full 36 hours had passed from injection to our care.
← Swipe to see more →
| Time | Event | Clinical Significance |
|---|---|---|
| T = 0 | HA filler injection (upper lip + nasolabial fold) at another clinic | — |
| T + minutes | Extensive bruising, swelling, pain, numbness — all simultaneous | The classic embolism red-flag triad |
| T + hours | Livedo reticularis (net-like red-purple) expanding | Visible sign of compromised arterial perfusion |
| T + 24 hours | Small pustules appearing along the nasolabial fold near the nose | Progressive ischemia, tissue damage emerging |
| T + 24-36 hours | Two days of high-dose extravascular hyaluronidase + HBOT at original clinic — failed | Extravascular flooding cannot reach intra-arterial plug |
| T + 36 hours | Friday 8 PM FB message to FILLER REVISION | Emergency intake by Dr. Liu |
| T + 44 hours | Saturday morning arrival, ultrasound + IAHA intervention | Rescue completed, symptoms stabilized |
| T + 2 weeks | Skin color and texture fully recovered | Penumbra successfully salvaged |
I had no scheduled clinic the next morning. I canceled my plans and waited for her specifically.
Because after filler embolism, what you're really fighting for is not just the already-injured or destined-to-die skin. It's the surrounding salvageable zone — the ischemic penumbra (tissue around the blocked vessel where blood flow is severely reduced but not yet zero; cells here can still be rescued with timely intervention, but will die if delayed). Do a little more, save a little more. Act a little earlier, lose a little less necrosis, leave a little less scar.
Why Ultrasound Guidance Can Rescue Embolism at 36 Hours
Penumbra Theory — Why Late-Window Rescue Can Still Work
Vascular embolism doesn't produce an all-or-none tissue outcome. The central zone (core) loses blood flow completely and becomes irreversibly necrotic within hours. But the penumbra surrounding that core retains reduced — not zero — blood flow. These cells live in a reversible/irreversible gray zone.
Traditional textbooks place the rescue golden window at 6-24 hours. But penumbra survival time has significant interindividual variation, depending on:
- Residual perfusion (whether collateral circulation partially compensates)
- Surrounding tissue metabolic rate (younger, healthier tissue burns more O2 but tolerates ischemia better)
- The nature of the obstructing material (non-crosslinked HA partially degrades on its own; highly crosslinked HA needs more aggressive intervention)
- Presence of secondary infection or inflammation that worsens the ischemic burden
In this case, even after 36 hours, her penumbra had not fully necrosed. The skin showed severe red-purple mottling and the area was expanding, but a capillary refill test (pressing on the skin and watching how quickly color returns — a microvascular function readout) showed the tissue was not yet at terminal-necrosis stage.
Further reading: Vascular Occlusion Mechanism & Emergency Response
Extravascular Flooding Failed — Why Intra-Arterial Hyaluronidase (IAHA) Worked
The original clinic had given her "two days of high-dose hyaluronidase + HBOT." Why did it fail?
The answer lies in where the hyaluronidase was delivered.
← Swipe to see more →
| Delivery Route | Mechanism | Best Suited For | Effective in This Case? |
|---|---|---|---|
| Extravascular flooding (subcutaneous, large-volume) | Hyaluronidase diffuses through surrounding tissue, gradually degrading filler from the outside in | Compression-type occlusion (filler external to the vessel, squeezing it shut); small embolism volumes | ❌ Cannot reach intra-arterial filler via tissue diffusion |
| Intra-arterial injection (IAHA, Intra-Arterial Hyaluronidase) | Hyaluronidase enters the obstructed artery directly, dissolving the intraluminal filler plug at its source | True intra-arterial embolism; failed extravascular flooding; delayed-window rescue | ✅ Direct source intervention |
This was an intra-arterial embolism — the filler had entered the lumen of a facial artery branch and plugged it. Extravascular hyaluronidase has to traverse tissue layers to reach the lumen, an extremely low-efficiency process. Worse, high-dose extravascular flooding also degrades the patient's own native HA in surrounding tissue, causing collateral damage (the well-documented cumulative damage from repeated dissolving).
Intra-arterial hyaluronidase (IAHA) is fundamentally different — under real-time ultrasound guidance, hyaluronidase is injected directly into the obstructed artery itself, contacting the filler plug along its blood flow path. Dissolution efficiency is orders of magnitude higher. This is why, even after the original clinic had exhausted extravascular hyaluronidase, IAHA could still salvage the penumbra at the 36-hour delayed window.
Anatomical Precision: Facial Artery Branches and Embolism Localization
When she arrived at the clinic, I used high-frequency ultrasound (15-50 MHz imaging that visualizes filler deposits and surrounding vasculature in real time) to map the facial artery branches around her nasolabial fold.
The nasolabial fold region is a high-risk zone — beneath this fold run the terminal branches of the facial artery:
- Superior labial artery — supplies the upper lip
- Inferior labial artery — supplies the lower lip
- Lateral nasal artery — supplies the side of the nose
- Angular artery — supplies the medial canthus, and anastomoses upward via the dorsal nasal artery to the ophthalmic artery
The clinical significance of this anatomy: a misdirected nasolabial fold filler injection can, in theory, retrograde-embolize through this connected arterial network all the way to the retinal artery, causing blindness. That's why my first question was about her vision — not paranoia, but the standard precaution dictated by this anatomy.
Under ultrasound, I traced the course of her facial artery branches and identified a suspicious intraluminal hyperechoic mass — the filler causing the obstruction.
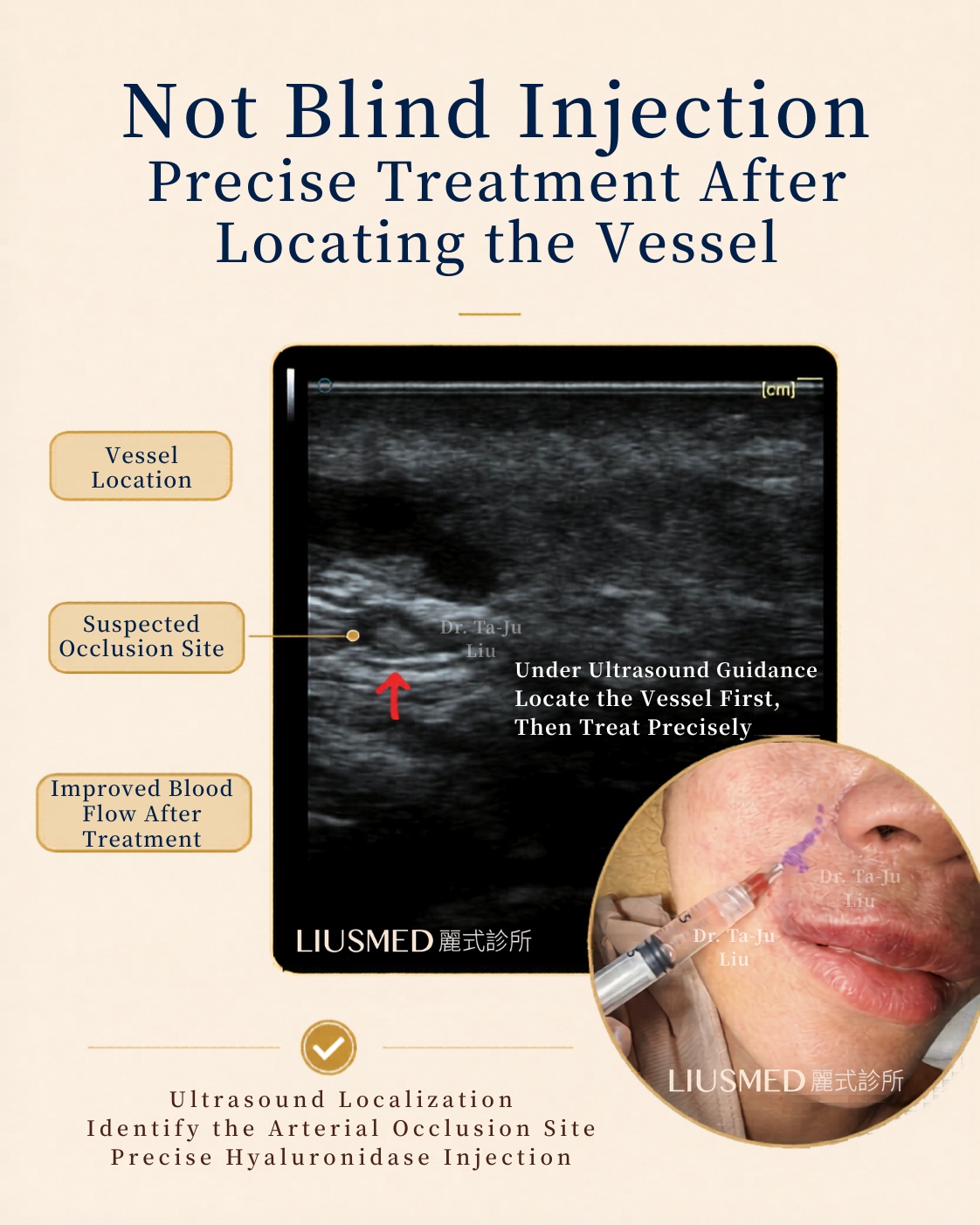
Under real-time ultrasound guidance, I performed intra-arterial hyaluronidase precision injection targeting the suspected obstruction and the ischemic regions around it — dissolving the HA plug inside the facial artery branch directly.
This is why I keep emphasizing: in this situation, the answer isn't "blind injection of more dissolver" or "just inject a lot of dissolver everywhere." What matters is: Where is the vessel? Where is the suspected obstruction? Is blood flow returning? Is there still penumbra to salvage?
As I watched her clinical status stabilize after the intervention, I told her with some relief:
"The most dangerous phase should be behind us."
She was still on the procedure table when she broke down sobbing. I could feel that she had held it together until the very last moment, and now finally let it all out. She told me how unbearable the past two days had been — terrified the skin would die and scar, terrified of losing her vision, terrified that the golden window had already closed.
I felt that deeply. With aesthetic medicine complications, the most exhausting part is often not the visible skin change — it's that endless dread of will this get worse, will my face be permanently damaged, will I be left with scars forever.
Warning Signs: What's Not Just a Bruise
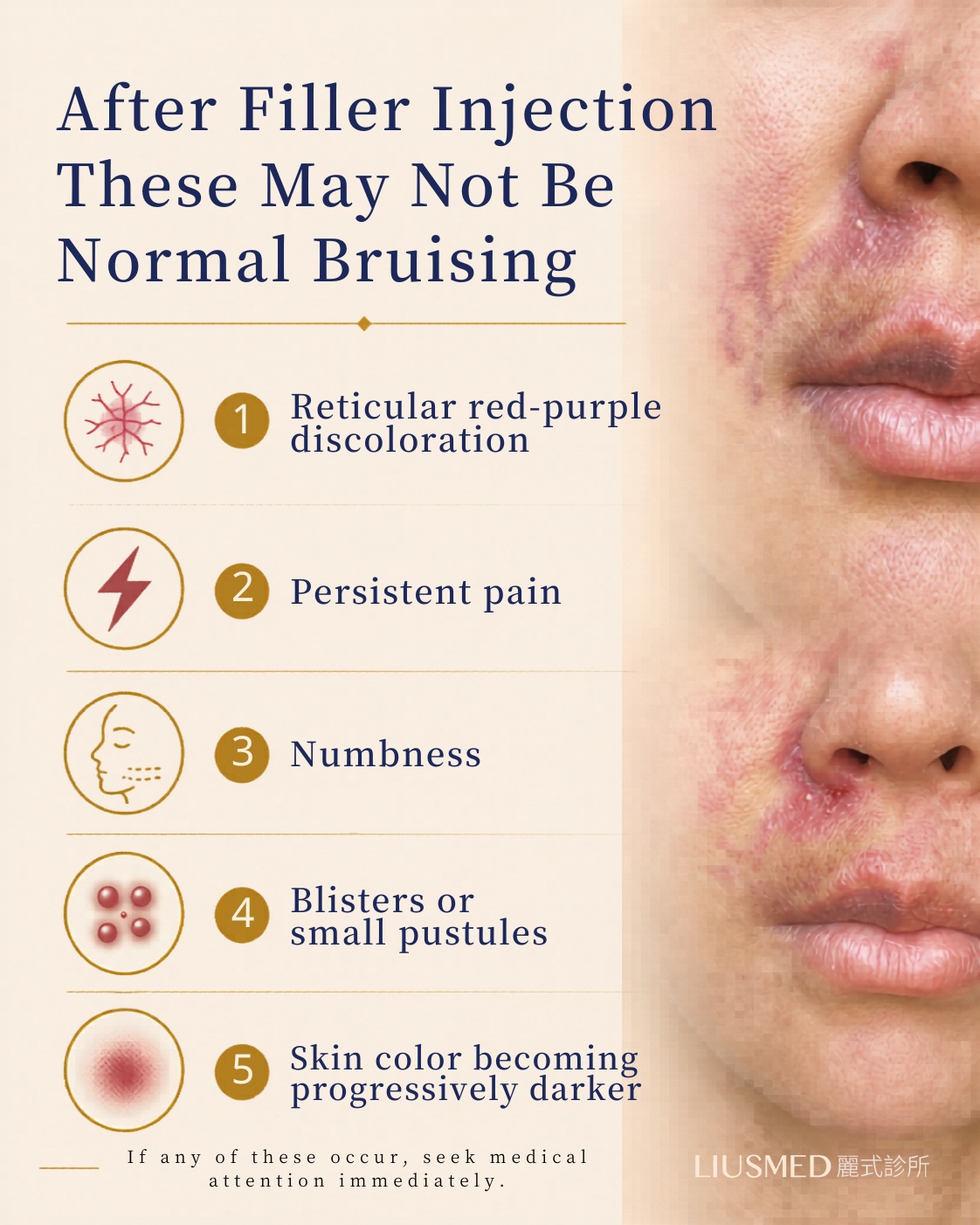
After a filler injection, if you see any of the following, do not dismiss it as ordinary bruising:
- Livedo reticularis — net-like, lacy red-purple mottling, distinct from the uniform solid discoloration of normal bruising
- Persistent or disproportionate pain — beyond the expected post-injection soreness
- Numbness — a sign of nerve ischemia
- Blisters or small pustules — superficial tissue damage
- Progressive worsening skin color — white → purple → black is the ischemia progression
- Blurred vision, eye pain, or any visual disturbance — the worst possible sign, indicating retrograde ophthalmic artery embolism
None of these are signs to "wait and see."
What NOT to do (intuitive but actively harmful):
- Apply ice to suppress symptoms — the vessel is already constricted; cooling makes ischemia worse. The correct response is warm or room-temperature compress to promote flow.
- Massage the area to "push out the bruise" — you'll spread the filler plug.
- "Let's see how it looks tomorrow" — the penumbra shrinks every hour. Delay directly determines how much tissue you can save.
- Photograph for evidence but don't seek care — photos matter, but seek care first, photograph en route.
What you SHOULD do:
- Contact the injecting physician immediately — call, message, any rapid channel
- If the injecting physician cannot intervene immediately or advises "just observe," find a revision specialty clinic with ultrasound-guided rescue capability — don't wait
- Photograph an hourly timeline as you go
- Bring the product box and lot number (this directly determines the right dissolution strategy)
- If any visual disturbance occurs, go directly to the emergency room — don't wait for any physician callback
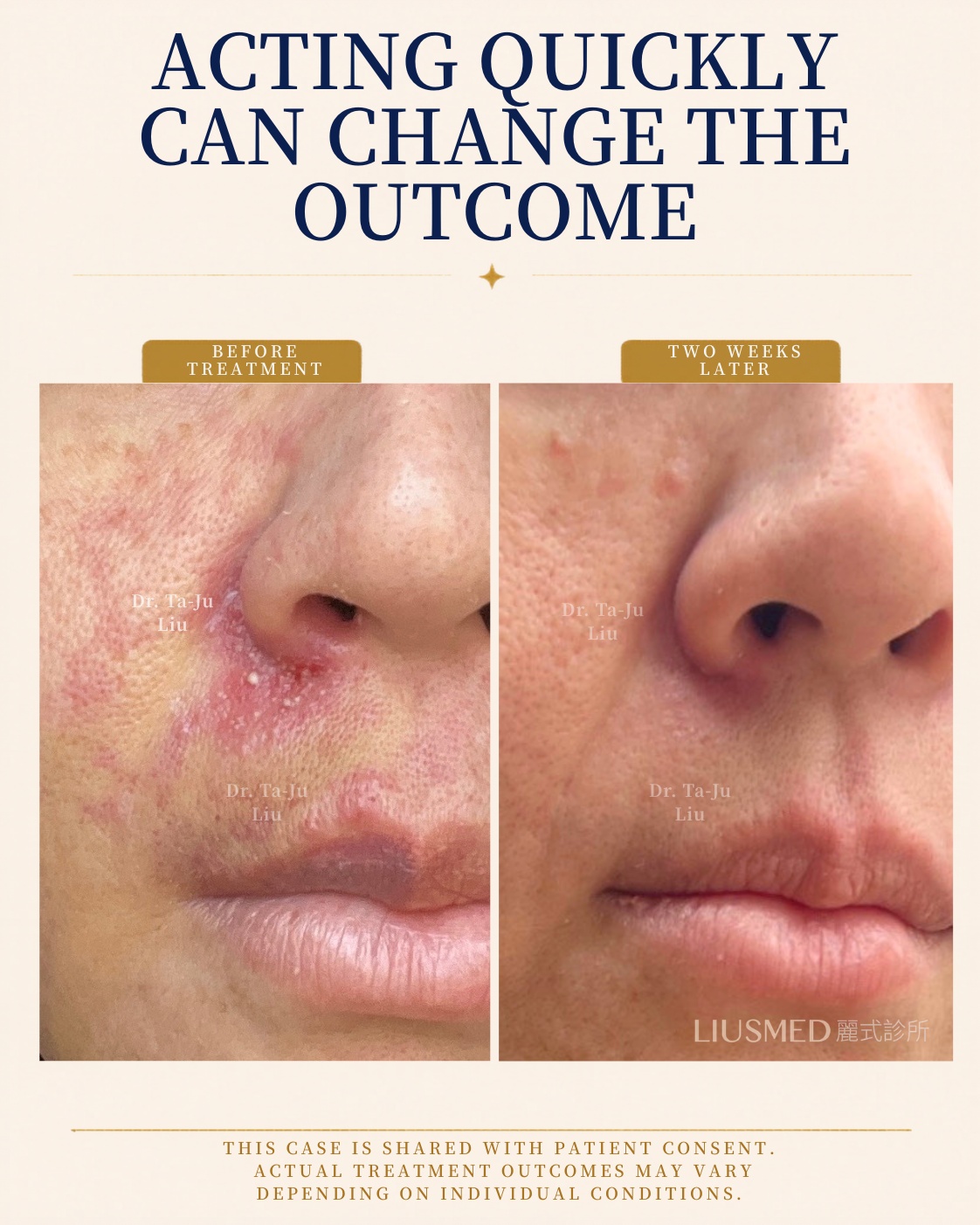
Two Weeks Later: Full Recovery
Two weeks later, she sent me photos. Her skin had recovered beautifully — no residual scarring. Only mild numbness remained in the upper lip (a common feature of peripheral nerve recovery after ischemia, typically resolving over 1-3 months).
Looking at those photos, I felt genuine relief. Because I knew that, somewhere in the middle of all this, we had done a little more:
- Asked one more question
- Looked at one more photo
- Used the ultrasound to actually find the vessel
- Saved a little more time
- Used IAHA to target the intra-arterial embolism source, after the original clinic had exhausted standard extravascular dissolution
And sometimes that "little more" is what changes a person's outcome.
Aesthetics can be adjusted slowly. Ischemia cannot wait.
I'm sharing this case not to make people fear hyaluronic acid. HA is a common and valuable filler treatment. But any injection treatment involving the facial vasculature carries risk, and the patient — and the physician — must know that risk and the warning signs.
This case is shared with the patient's full informed consent. Actual treatment approach and recovery outcomes depend on each patient's individual situation, timing, injection location, and degree of ischemia. The successful rescue at a 36-hour delayed window in this case does not mean every case can replicate this outcome — earlier intervention is always better.
When You Should Seek Care Immediately
If you or a family member has just had a filler injection and develops any one of the following:
- Net-like red-purple discoloration + abnormal persistent pain (two or more co-occurring)
- Skin color persistently darkening or expanding (not gradually fading)
- Any visual disturbance (blurring, dimness, visual field defects, eye pain)
Seek emergency care immediately — the sooner the better. Do not wait until tomorrow. Do not wait for the weekend to pass.
If the original clinic cannot manage the case, or symptoms continue to worsen after their intervention, see:
- Vascular Occlusion Repair Service — FILLER REVISION's emergency protocol
- Vascular Occlusion Mechanism & Emergency Response — detailed pathophysiology and management principles
- Facial Anatomy Danger Zones — highest-risk injection sites
- Why Hyaluronidase Fails: 7 Reasons — what to do when extravascular dissolution doesn't work
- Contact for Consultation — non-emergency consultation booking
Frequently Asked Questions
Q1: Traditional teaching says the rescue golden window is the first 6 hours. Is 36 hours still rescuable?
A: The "golden window" is a statistical best-intervention period — not an absolute death-line. Tissue survival actually depends on the penumbra's status, and penumbra viability varies between individuals depending on residual perfusion, collateral circulation, and tissue metabolic rate. This case succeeded at 36 hours because: (1) the penumbra had not fully necrosed; (2) ultrasound-guided IAHA precisely targeted the source; (3) the original clinic's HBOT, though not curative, slowed the ischemic progression. None of this means you should delay — earlier intervention is always better.
Q2: Why did two days of high-dose hyaluronidase + HBOT at the original clinic fail?
A: Because neither can directly reach the intra-arterial filler plug. Extravascular hyaluronidase has to diffuse through tissue layers to reach the vessel lumen — for true intra-arterial embolism, this is extremely inefficient. HBOT can increase tissue oxygen delivery and slow ischemic progression, but it does not remove the vascular obstruction itself. Intra-arterial hyaluronidase injection (IAHA) is the primary modality that directly targets the source — under ultrasound guidance, hyaluronidase is delivered into the arterial lumen and dissolves the filler along the blood flow.
Q3: How can I tell if post-filler bruising is normal or actually an embolism?
A: Look at three dimensions: (1) Distribution — embolism produces net-like, lacy livedo reticularis; ordinary bruising is uniform solid discoloration. (2) Time progression — embolism expands or darkens; bruising fades over time. (3) Associated symptoms — embolism often comes with disproportionate pain, numbness, decreased skin temperature, and slow capillary refill. If in any doubt, treat it as embolism — a false alarm is far better than missing a true emergency.
Q4: Which injection sites have the highest embolism risk?
A: By documented incidence, from highest to lower: (1) Glabella — terminal vasculature with poor collateral compensation; (2) Nose (dorsum, ala) — direct anastomosis to ophthalmic system, highest blindness risk; (3) Nasolabial fold — the site in this case, with the angular artery running beneath; (4) Upper / lower lip — direct labial artery involvement; (5) Temple / temporal region — high anatomical variability. All facial injection carries risk, but these sites demand higher anatomical knowledge and ultrasound capability. Further reading: Facial Anatomy Danger Zones.
Q5: If I notice embolism signs, what should I do first?
A: Four steps: (1) Contact the injecting physician immediately, demand immediate treatment; (2) If they can't intervene now or advise "observe," actively seek a revision specialist with ultrasound-guided rescue capability — do not wait; (3) Photograph an hourly timeline, bring the product box and lot number; (4) If any visual disturbance appears, go directly to the emergency room — do not wait for any physician callback. Remember: aesthetics can be adjusted slowly, but ischemia cannot wait.
Q6: Why was FILLER REVISION able to rescue this case at the 36-hour delayed window?
A: Three capabilities had to come together: (1) Real-time ultrasound guidance — to actually see facial artery branches and identify intraluminal filler plugs under imaging; (2) Intra-arterial hyaluronidase (IAHA) technique — to deliver dissolution directly into the artery, rather than flood the surrounding tissue; (3) Rapid response workflow — Dr. Liu canceled his Saturday plans to wait for the patient's arrival. All three are necessary. This is also why embolism rescue requires a revision specialty clinic with dedicated equipment, technique, and workflow.
Q7: How can I tell if my injector or rescue clinic actually does ultrasound-guided IAHA?
A: Ask three direct questions: (1) "Do you have a high-frequency ultrasound machine on-site, and can you show it to me?" — emergency IAHA needs 15-50 MHz imaging actually present in the room, not "we'll refer you out." (2) "Have you personally performed IAHA on a vascular occlusion case before?" — case volume matters; ask for outcome details, not just yes/no. (3) "What's your protocol if extravascular hyaluronidase fails?" — if they only describe more extravascular flooding or HBOT, they are not doing IAHA. A clinic equipped for IAHA will describe ultrasound mapping of facial artery branches, intra-arterial needle placement, and direct intraluminal hyaluronidase delivery. If the answers feel vague, that itself is your answer — go elsewhere.
Q8: How long does it take and what does it cost to find a clinic that does IAHA?
A: Honest answer: emergency IAHA capacity is rare globally. Most cosmetic clinics — even ones that injected your filler — do not have on-site ultrasound or the experience to perform intra-arterial injection. Time matters more than cost. Practical priorities: (1) Call ahead to confirm ultrasound is on-site and the physician can see you within the next 2-4 hours; do not just show up. (2) Costs vary widely — emergency vascular rescue may run USD 1,000-5,000+ depending on region, hyaluronidase volume needed, and follow-up imaging; insurance typically does not cover cosmetic complications. (3) Travel matters less than you think — even 2-3 hours of travel is acceptable if it gets you to genuine IAHA capability rather than a closer clinic that will only repeat extravascular flooding. The limiting resource is salvage time, not money.
Q9: After surviving a vascular embolism, can I ever safely have filler again — even years later?
A: Many patients do return to filler — but only with significantly modified safety protocols and ideally not in the same anatomical region. The decision rests on three factors: (1) Why the original embolism happened — technique error, anatomical variation, or a high-risk site like the glabella or nose; an anatomical variation that caused it once can cause it again. (2) The new injector must use ultrasound guidance — after a vascular event, ultrasound-guided injection is no longer optional. Any clinic that says "we don't need ultrasound" is automatically the wrong choice. (3) Pre-injection vascular mapping is essential — before the new injection, the injector should sonographically map your facial artery branches and identify any residual filler from the prior incident. At FILLER REVISION, we perform this evaluation for any patient with a prior vascular event before considering re-injection. For some patients, the safer choice is to avoid injectable fillers entirely and use surgical or non-injectable alternatives.
Author: Dr. Ta-Ju Liu (FILLER REVISION Repair Specialty) Specialty: Ultrasound-guided filler revision and vascular embolism emergency intervention