
Post-Vascular Occlusion Repair
"The Emergency Is Over, but My Skin Is Still Black — Then I Was Abandoned"FILLER REVISION's Multimodal Reconstruction Starts Where Others Stopped
"The day my skin turned black, the ER injected hyaluronidase. Two weeks later, the doctor said the vessel was open and the acute phase was over — but the dark patch and indented scar on my face, he said I could only wait. Three months later, nothing had changed." At FILLER REVISION, cases like this — abandoned after acute rescue — account for over 80% of our post-occlusion repair consultations. Dr. Liu integrates five core technologies — hyperbaric oxygen, photobiomodulation, regenerative medicine, and more — providing systematic active reconstruction specifically for patients told "nothing more can be done" about their post-occlusion sequelae.
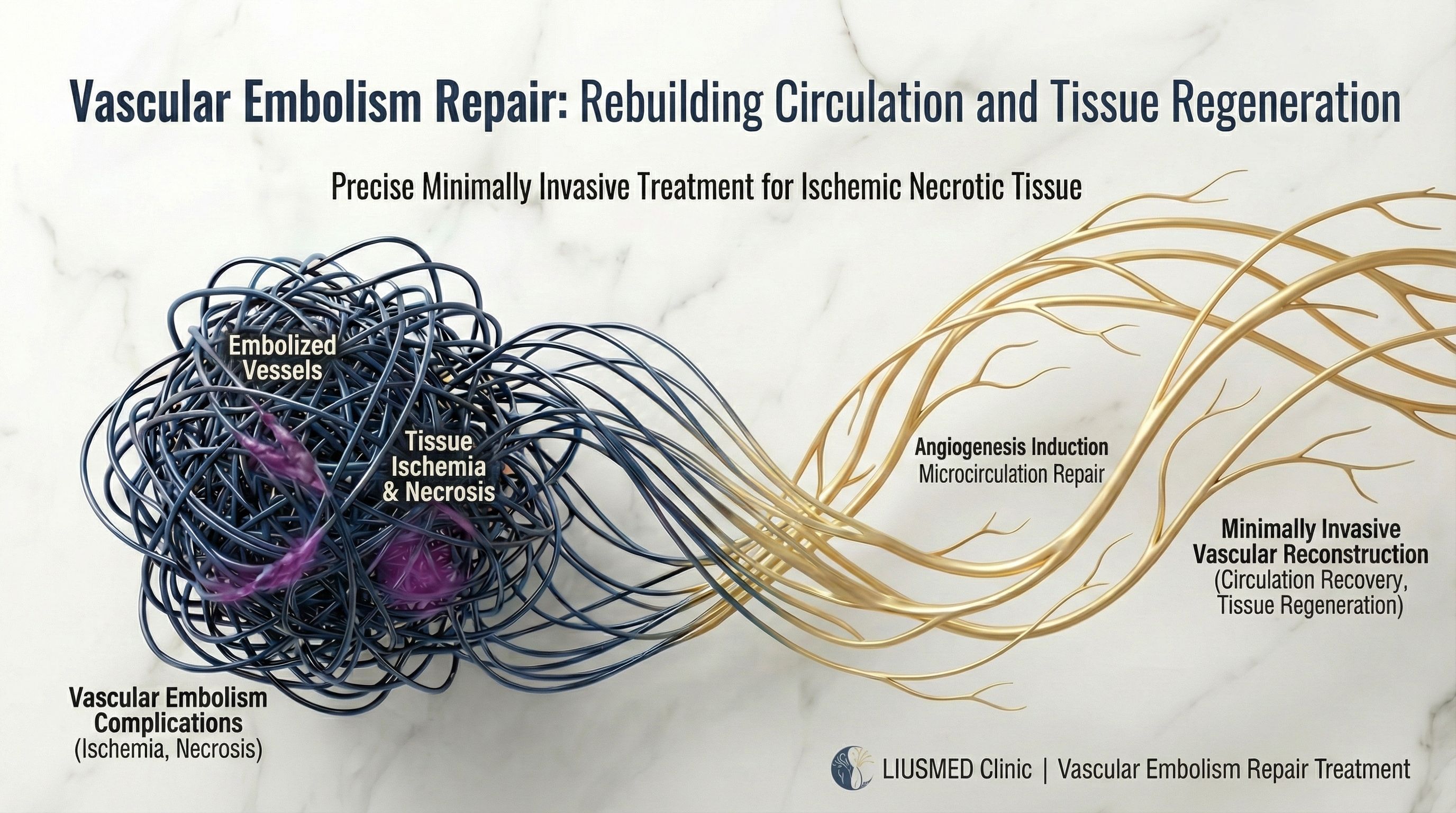
Table of Contents
After Occlusion, Are You Facing These Problems?
Even after acute-phase treatment, these sequelae may continue to affect your appearance and quality of life:
Common Post-Occlusion Sequelae
"The emergency was over, the doctor said just wait — three months later, the dark patches and scars hadn't budged." At FILLER REVISION, we take on these "abandoned after acute rescue" cases every day. Waiting was never treatment — active intervention is.
Pathology: Three Injury Mechanisms
Understanding injury mechanisms explains why "multimodal" simultaneous treatment is needed, not a single approach.
Ischemic Penumbra
The Salvageable Gray Zone
Tissue in the central occlusion zone dies from complete ischemia, but a surrounding "penumbral zone" exists where blood flow is severely reduced but not completely interrupted. These tissues still have a chance of survival but will gradually die over time. The goal of active intervention is to rescue this penumbral tissue.
Reperfusion Injury
Secondary Damage After Blood Flow Returns
After blood flow resumes, a surge of oxygen free radicals and reactive oxygen species (ROS) floods in, causing "secondary damage" to already fragile tissue. Simultaneously, inflammatory cells aggregate and release cytokines, triggering severe inflammatory cascades. This is why simply restoring blood flow is insufficient — complementary anti-oxidant and anti-inflammatory treatments are essential.
Double Hit Theory
Synergistic Effect of Ischemia + Reperfusion
The first hit is direct damage from ischemia itself; the second hit is reperfusion injury from free radicals and inflammation after blood flow returns. The combined destructive force far exceeds the sum of each independently. This explains why post-occlusion sequelae are more severe than expected, and why "multimodal" simultaneous intervention is essential — no single treatment can address this compound injury.
Golden Watershed: HA vs Non-HA Rescue Strategy
The chemical nature of the filler determines the recovery pathway — the availability of an "antidote" is the critical difference.
Hyaluronic Acid (HA) Occlusion
- Hyaluronidase can be used for acute dissolution
- If the golden rescue window is missed or dissolution incomplete, multimodal repair is still required
- Sequelae repair focus: antioxidation, microcirculation rebuild, tissue regeneration
Non-HA Filler Occlusion
CaHA (Radiesse), PLLA (Sculptra), PCL, etc.
- Cannot be dissolved by enzymes — no "antidote" exists
- Only option is aggressive multimodal supportive therapy to salvage tissue
- Requires even earlier and more comprehensive repair intervention
Dead Ends of Passive Recovery
These are common but limited traditional approaches that cannot address the root problem of post-occlusion injury:
Wait and Observe
Misses the golden repair window — tissue damage progresses, hyperpigmentation and scarring only become harder to treat.
Steroid Injection
May temporarily suppress inflammation but cannot address the root cause of ischemic damage; long-term use causes skin atrophy.
Premature Laser Treatment
Applying laser before tissue is fully repaired may worsen damage, delay healing, and even create new pigmentation issues.
Topical Ointments
Topical application cannot penetrate to damaged deep tissue layers; extremely limited effect on post-ischemic microcirculation disorders.
Five Repair Modalities
Systematically integrating five treatment modalities, from vascular repair to tissue regeneration
Functional Microcirculation Repair IV
Precision Formula + Acute Repair + Microcirculation Rebuilding
Not a regular "beauty drip" — this is a therapeutic infusion designed for occlusion injuries. Simultaneously dilates vessels, optimizes microcirculation, and neutralizes free radicals from ischemia. Used intensively during the golden repair window to create favorable conditions for tissue recovery.
Hyperbaric Oxygen Therapy (HBOT)
Deep Oxygenation + Bypass Blockage + Revive Dying Tissue
"Dissolving" oxygen into blood — like bubbles in soda. Under pressure, oxygen reaches oxygen-starved areas without needing red blood cells, sustaining dying cells and promoting new vessel growth. Research shows effectiveness even when started 5 days post-occlusion.
Photobiomodulation (PBM/LLLT)
Light Energy Repair + Cellular Recharge + Accelerated Healing
Perfectly complementary to HBOT — if HBOT "delivers fuel" to cells, photobiomodulation "starts the engine." Medical-grade red and near-infrared light at specific wavelengths penetrate deep into tissue, reactivating the energy production systems of damaged cells — like recharging a dead phone battery. Once cells regain energy, they can accelerate self-repair: promoting collagen synthesis, accelerating fibroblast proliferation, and significantly improving wound healing speed and quality.
Regenerative Medicine
Autologous Repair + Growth Factors + Tissue Reconstruction
Harnessing your body's own repair power — we extract high concentrations of growth factors and repair signaling molecules from your own blood, injecting them into damaged areas to guide tissue reconstruction. These natural repair factors accelerate new blood vessel formation, promote healthy tissue growth, and reduce fibrotic scarring. For more severe tissue defects, we can employ advanced stem cell technology, utilizing regenerative cells from your own tissue to provide even more powerful repair and anti-inflammatory capabilities for more complete tissue reconstruction.
Advanced Wound Care
Scientific Dressing + Moist Healing + Scar Minimization
Modern wound care has abandoned the outdated "keep dry and scabbed" approach, adopting clinically proven "moist wound healing" principles — accelerating skin regeneration and dramatically reducing scar formation. Our medical team precisely selects the most appropriate professional dressings and care protocols for each stage of wound repair, combined with regenerative medicine techniques, ensuring every healing phase proceeds under favorable conditions to achieve the ultimate goal of scar minimization.
FAQ
Can skin that turned black after vascular occlusion still be saved?
Yes. Skin darkening indicates the area is in an ischemic state, but it does not mean the tissue has necrosed. With aggressive multimodal repair treatment within the golden rescue window, there is still a chance to restore blood flow and salvage tissue. The key is early intervention.
How is post-occlusion repair different from acute dissolution rescue?
Acute rescue is emergency treatment within the first hours after occlusion. Our post-occlusion repair targets patients who, after the acute phase, have experienced ischemic injury and developed complications like hyperpigmentation, ulceration, or scarring, providing systematic multimodal reconstruction.
Why is hyperbaric oxygen therapy effective for post-occlusion repair?
HBOT increases dissolved oxygen in plasma by 10-15 times, delivering oxygen to ischemic tissues without relying on red blood cells. Particularly important for areas where blocked blood vessels prevent red blood cells from reaching, effectively supporting tissue survival and regeneration.
How long does the repair treatment take?
Depends on damage severity. Mild hyperpigmentation may improve in 2-4 weeks, moderate ulceration requires about 4-8 weeks of intensive treatment, and severe scarring may need months of staged repair. Costs are individually quoted after the doctor's detailed assessment.
Can post-occlusion repair fully restore the original appearance?
Recovery depends on initial injury severity, intervention timing, and individual healing capacity. Mild ischemic injuries can often achieve near-complete recovery; moderate to severe injuries aim for maximum functional restoration. We honestly assess expected improvement range during initial consultation.
Why can't I just "wait and observe"?
Post-ischemic tissue faces the double hit of reperfusion injury — even when blood flow partially returns, free radicals and inflammation continue damaging tissue. Passive waiting misses the golden repair window and may deepen hyperpigmentation and worsen scar contracture. Active multimodal intervention is needed to interrupt the injury cascade.
I had acute occlusion treatment at another hospital, but the sequelae have not improved. Is there still hope?
Yes. The vast majority of our post-occlusion repair patients are those who had acute rescue at other institutions but came seeking a second opinion because their sequelae persisted. Acute dissolution or rescue only addresses the "vessel recanalization" step, but the ischemic tissue injury, reperfusion injury, hyperpigmentation, and scar formation all require subsequent systematic multimodal repair to truly improve. Regardless of how long ago the occlusion occurred, as long as the tissue retains repair potential, we can design a targeted reconstruction plan.
It's been six months since the occlusion. The dermatologist said the scar is stable and can't improve further — is that true?
From a traditional dermatology perspective, a "stable" scar means it won't change on its own. But "won't improve on its own" and "cannot be improved" are entirely different concepts. FILLER REVISION's integrated multimodal repair — HBOT promoting deep neovascularization, PBM activating cellular repair signals, regenerative medicine providing tissue reconstruction substrates — these active interventions can restart repair mechanisms that have stalled. We've treated patients who came a year or more after occlusion, and after systematic multimodal treatment, hyperpigmentation and atrophic scarring still showed significant improvement. The key isn't "how long it's been stable" — it's "whether the right approach was used."
Repair Process
Systematic assessment, multimodal integration, ongoing follow-up
Comprehensive Assessment
Detailed review of occlusion timeline, acute treatment history, current damage status, assessing tissue viability and repair potential
Multimodal Plan Design
Based on injury severity and type, integrate HBOT, IV therapy, PBM, regenerative medicine to create a personalized repair plan
Intensive Repair Phase
Initiate intensive treatment cycles with multiple modalities working synergistically, regularly assessing tissue response and dynamically adjusting the plan
Follow-up & Reconstruction
After acute repair stabilizes, enter long-term follow-up and tissue reconstruction phase, performing refined repair for residual scarring or pigmentation
Dr. Ta-Ju Liu
Director, Liusmed Clinic · Minimally Invasive Surgery Specialist
Specialties
Credentials
- 20+ years of minimally invasive surgery experience
- One of few Taiwan specialists focused on injectable complication repair
- Experienced in multimodal repair therapy integration
"Eight out of ten post-occlusion patients who come to FILLER REVISION were told to 'just wait.' But waiting won't regenerate necrotic tissue — we integrate five treatment modalities precisely so that waiting is no longer the main option."
Other Repair Services
Recovery after occlusion is not about waiting — it's about action.
Let evidence-based medicine provide the strongest support for your recovery.
References
- DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600.
- Beleznay K, et al. Vascular compromise from soft tissue augmentation: experience with 12 cases and recommendations for optimal outcomes. J Clin Aesthet Dermatol. 2014;7(9):37-43.
- Goodman GJ, et al. Current management of vascular occlusion following aesthetic procedures. J Cosmet Dermatol. 2021;20(9):2619-2628.
The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Case
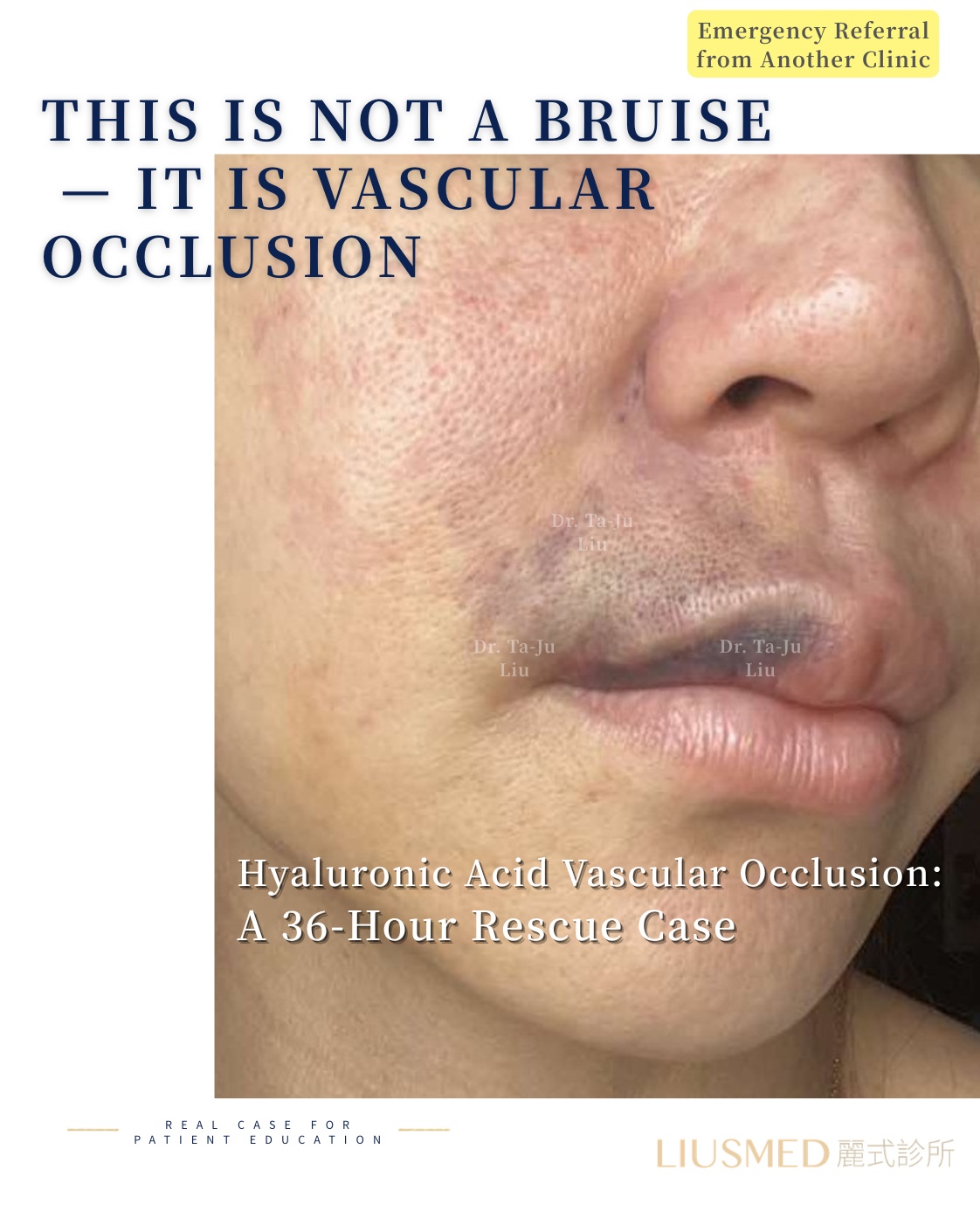
36 hours later — can it still be rescued?
"Referred after two days of failed extravascular hyaluronidase + HBOT at another clinic. Ultrasound-guided intra-arterial hyaluronidase (IAHA) precision injection — full recovery at two weeks."
Hours of delay
Days to recovery
Featured Poster
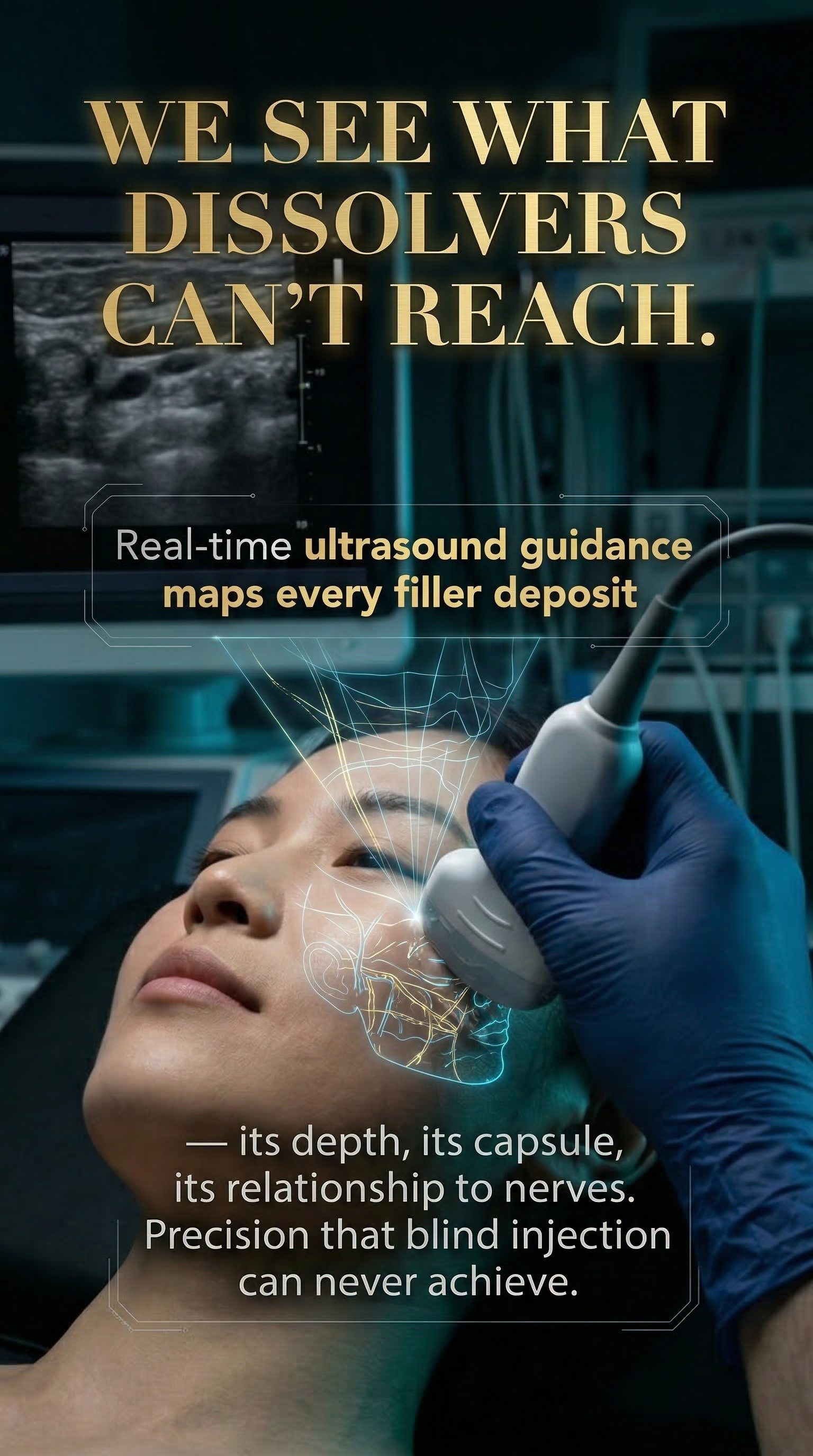
We see what dissolvers can't reach.
Real-time ultrasound guidance maps every filler deposit — its depth, its capsule, its relationship to nerves.
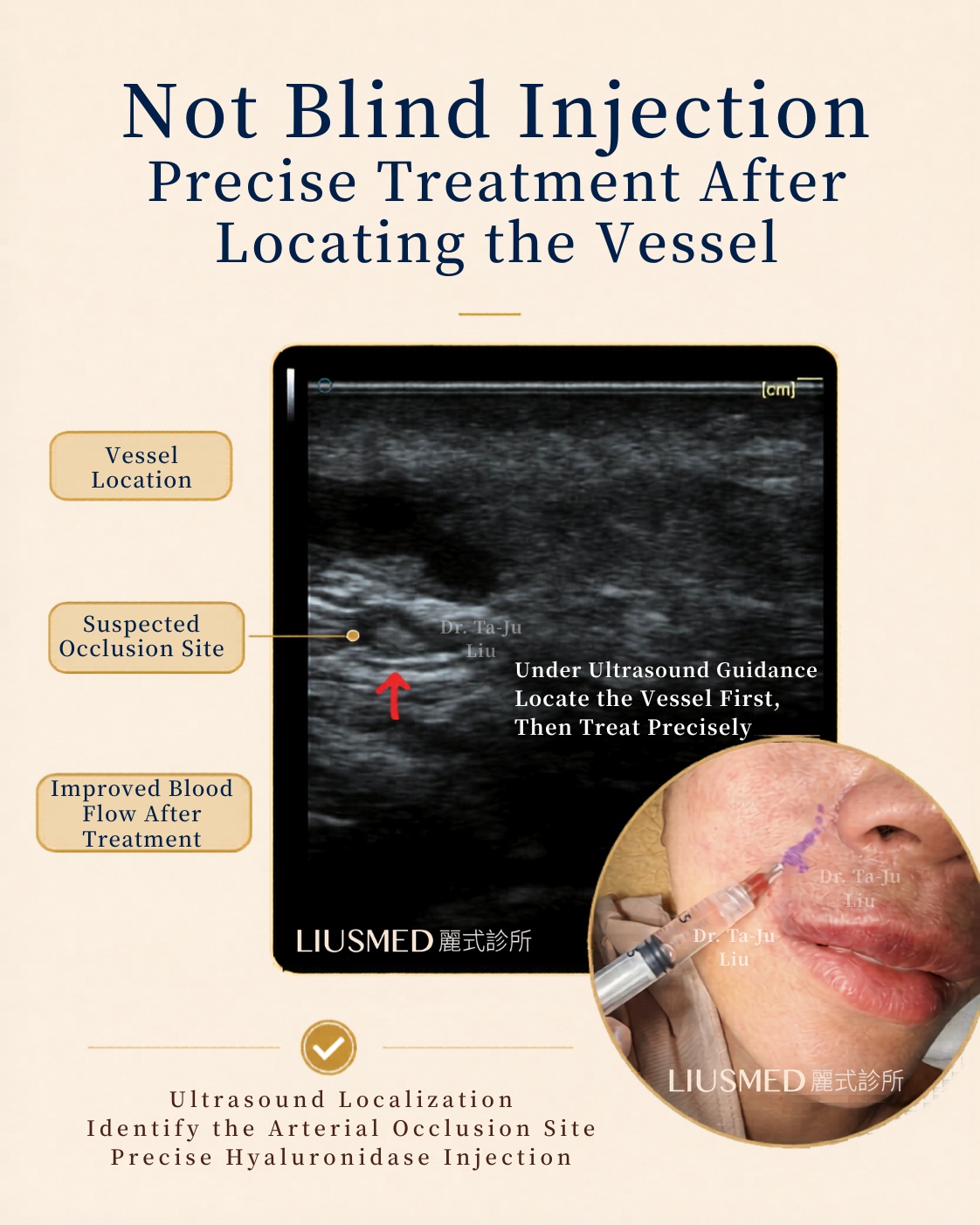
Not blind injection — find the vessel first, then treat precisely.
Under real-time ultrasound: localize the occlusion, then deliver intra-arterial hyaluronidase exactly where it's needed.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
"Abandoned After Emergency Rescue" — FILLER REVISION Restarts Where Others Stopped
Over 80% of our post-occlusion patients were told to "just wait" after emergency treatment — and waited with no improvement
Every day of passive waiting after ischemia, reperfusion damage accumulates further. Book a FILLER REVISION post-occlusion specialist evaluation now — replace passive waiting with active intervention
Book Consultation