
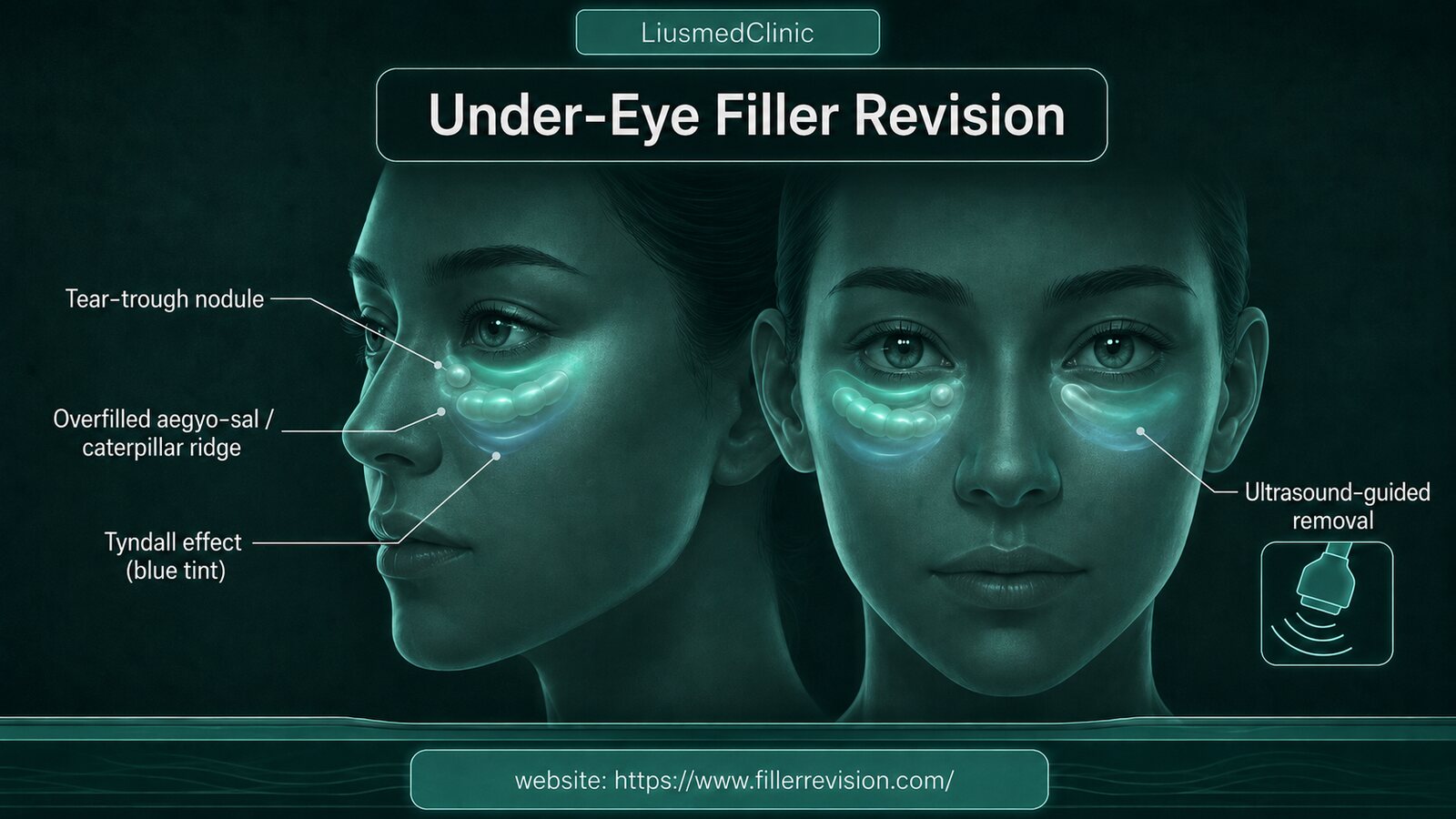
Tear-Trough & Aegyo-Sal Filler Nodules and the Caterpillar Under-Eye
'I had HA put in my tear troughs — so why is the area underneath puffier now, turned into a caterpillar?' 'The more aegyo-sal filler I add, the bigger it gets — smiling, it looks like two meatballs hung under my eyes.' That's how many people arrive. The under-eye is the thinnest, least forgiving skin on the whole face — and the problem here is usually not too little volume, it's structure and position. Beneath the tear trough runs a layer of tissue called the malar septum, which separates the eye area from the cheek; HA injected here draws water, and with that septum blocking lymphatic return, the interstitial fluid can't drain, so it turns into puffiness that won't go away and aegyo-sal that becomes an eye-bag (many people describe it as a caterpillar or a meatball). Placed too superficially it shows a bluish tint (the Tyndall effect); placed too deep or in too much volume it migrates, hardens into lumps, even a granuloma. What I want to ask first is: did anyone use high-frequency ultrasound before touching it — to see whether this is HA that can still be dissolved, an encapsulated lump, migration, or a granuloma? Which layer it's in, and how close to the vessels? Only once you can see it clearly can you decide whether to loosen it, move it, or remove it precisely — rather than adding another syringe or blindly injecting more hyaluronidase.
Common Symptoms
Why tear-trough and aegyo-sal filler grows puffier — and turns into a caterpillar
The under-eye has the thinnest skin on the whole face, with little subcutaneous space and a rich supply of vessels and lymphatics — the margin for error is very low. Between the tear trough and the cheek runs the malar septum, a relatively impermeable barrier; HA draws water, so once injected under the eye it absorbs fluid, and with the septum blocking lymphatic return and the interstitial fluid unable to drain, it forms puffiness that won't go away — the aegyo-sal is stretched out and the lower lid bulges, looking just like a caterpillar or a hung meatball. Because the skin is so thin, placing it even slightly too superficially shows a bluish tint (the Tyndall effect); too much volume or too deep a placement migrates easily and gets encapsulated into nodules. Biostimulators (PCL, PDLLA, CaHA) and permanent fillers have no dissolving enzyme and can remain for many years. None of this is solved by 'just adding a little more' — you first have to see which layer the material is in, and whether what it's causing is edema or a hard lump.
Why Traditional Treatments Fail
Why 'add more' and 'keep injecting hyaluronidase' are especially risky under the eye
The under-eye skin is thin and the margin for error is low, so the two most common moves — adding a bit more, or repeatedly injecting hyaluronidase — are both especially prone to trouble here. Adding more: under-eye puffiness is often caused by HA drawing water plus lymphatic fluid that can't drain, so more volume only makes it puffier. Hyaluronidase: it only works on HA, and lumps sealed in a thick capsule often won't dissolve cleanly; and because the under-eye skin is so thin, repeated enzyme injections without careful dosing tend to dissolve the surrounding normal tissue too, leaving the already-thin lid laxer and more crepey. Biostimulators and permanent fillers have no enzyme at all. If it's a granuloma, the inflammation has to be controlled first rather than being forcibly aspirated. The problem is usually not 'not enough' — it's not having distinguished first whether this is edema, a hard lump, migration, or actually your own fat herniation.
“The most heartbreaking thing about the under-eye is when you only wanted to improve the tear trough and ended up with a caterpillar that won't go away. The skin here is the thinnest and the lymphatics clog easily, so the moment HA draws water it swells up — and more filler or more anti-inflammatories won't help. The real question to ask is: did anyone use ultrasound before touching it, to see clearly whether this is edema, a lump, migration, or actually your own fat? Once you can see it, then decide whether to loosen, dissolve, or remove — that's far more honest than endlessly adding volume in the most fragile place on the face.”
Dr. LiuStructure > volume: the under-eye is the thinnest area — see it first, then decide to loosen, move, or remove
Ultrasound-Guided Pinhole Micro-Extraction
The under-eye isn't fill-it-when-sunken, dissolve-it-when-swollen. The skin here is the thinnest, the lymphatics and vessels the densest, the margin for error the lowest — so we build trust on imaging: ultrasound first tells whether this is puffiness from HA drawing water, an encapsulated lump, migration, or your own fat, then we decide whether to loosen, dissolve, or remove precisely. We're not trying to fill the under-eye up — we bring the caterpillar and meatball back to natural while protecting that thin layer of eyelid skin.
Tell edema, lump, or fat apart first
An under-eye bulge could be puffiness from HA drawing water with blocked lymphatics, a migrated nodule, a granuloma, or your own infraorbital fat — ultrasound objectively tells which layer it's in, so we don't treat in the wrong direction.
Loosen what can be dissolved, single-pinhole removal for the rest
HA that isn't yet encapsulated is dissolved precisely under ultrasound guidance, releasing the volume holding it up; material sealed in a thick capsule, and biostimulators and permanent fillers with no enzyme, are removed precisely through a single-pinhole micro-approach under image guidance; a granuloma has its inflammation controlled first.
In the thinnest place, gentle and staged
The under-eye skin is the thinnest, so we pay particular attention to layers and gentleness — we'd rather be cautious and work in stages to leave the layers smooth than make the thin lid laxer and more crepey chasing 100%.
Ultrasound-guided: tell whether it's edema, a lump, or fat first, then decide to loosen, dissolve, or remove
With the under-eye, the key is to see it clearly first. Before anything, high-frequency ultrasound tells whether what you feel is puffiness from HA drawing water, an encapsulated lump, migrated filler, a granuloma, or actually your own infraorbital fat herniation — which layer it's in, and how close it sits to the rich under-eye vessels and lymphatics. Once it's clear, we triage: HA that isn't yet encapsulated is dissolved precisely under ultrasound guidance, releasing the volume that was holding the fluid in place; material sealed in a thick capsule, along with biostimulators and permanent fillers that can't be dissolved, is removed precisely through a single pinhole under image guidance (clinically most of it, roughly 80–90%, depending on fibrosis); a granuloma has its inflammation controlled first. Because the skin here is the thinnest, removal calls for particular gentleness and attention to layers — the goal is to bring the under-eye back smooth and return the caterpillar and meatball to how they were, rather than leaving the thin lid laxer.
High-frequency ultrasound to tell edema, lump, or fat
Comfort-focused local anesthesia
Dissolve precisely what can be reached, single-pinhole removal for the rest
Finished gently and smooth, protecting the thin lid
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
Not necessarily — this is very common under the eye. Beneath the tear trough the malar septum blocks lymphatic return, and HA draws water, so the interstitial fluid can't drain and forms puffiness that won't go away. This kind of swelling usually doesn't respond to more filler, warm compresses, or anti-inflammatories, because the problem is the filler volume holding it up. Ultrasound first shows whether it's this kind of edema, a lump, or migration, so we can decide whether to loosen it, dissolve it, or remove it.
It can be assessed. An overfilled aegyo-sal that stretches out and droops, looking like a caterpillar or a meatball, usually comes from too much volume placed too superficially. Ultrasound first locates which layer it's in and whether it has clumped, then the excess and migrated portions are precisely reduced and removed to bring the aegyo-sal back to a natural curve — rather than adding another syringe to try to cover it.
It depends on the material and whether it's encapsulated. Only HA has a matching enzyme, and when it's sealed in a thick capsule it often won't dissolve cleanly; and because the under-eye skin is so thin, repeated enzyme injections without careful dosing tend to dissolve the surrounding normal tissue too, leaving the lid laxer and more crepey. Biostimulators (PCL, PDLLA, CaHA) and permanent fillers have no dissolving enzyme, so for those stubborn lumps ultrasound-guided physical removal is the more direct route.
That's exactly why ultrasound comes first. An under-eye bulge could be puffiness from filler drawing water, a migrated nodule, or your own infraorbital fat herniation (a true eye-bag) — the treatments are completely different. Ultrasound objectively distinguishes filler from fat and which layer it's in, so filler that should be removed isn't mistaken for an eye-bag, and fat isn't forcibly dissolved as if it were filler.
The Tyndall effect is the bluish tint that appears when HA is placed too superficially and light refracts through the thin skin. Under-eye skin is the thinnest on the face, so it's especially prone to this. It usually needs the too-superficial HA dissolved or removed precisely, rather than trying to cover it with more filler or laser.
Our aim is to remove cleanly and evenly, but clinically it's usually around 80–90%, depending on how much fibrosis there is — we don't claim 100%. The under-eye skin is the thinnest, so we'd rather be cautious and work in stages, leaving the layers smooth and protecting the thin lid, than injure the surrounding tissue chasing 100%.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Frankeny A. Dissolving vs. removing fillers in the nose prior to rhinoplasty. American Society of Plastic Surgeons (ASPS) — interview with Richard Reish, MD, FACS (notes that large volumes of the enzyme can cause damage to the surrounding tissues).
- Karlin J, Vranis N, Dayan E, Parsa K. Post-Hyaluronic Acid Recurrent Eyelid Edema: Pathophysiologic Mechanisms and a Proposed Treatment Protocol. Aesthetic Surgery Journal Open Forum. 2023;5:ojad102. (Describes the malar septum as a relatively impermeable barrier and notes that compromised lymphatic drainage from HA filler slows interstitial fluid clearance.)
- Ianhez M, de Goés E Silva Freire G, Sigrist RMS, et al. Complications of collagen biostimulators in Brazil: Description of products, treatments, and evolution of 55 cases. J Cosmet Dermatol. 2024. (Lumps in 89.1% of 55 cases, complete resolution in only 9.1%, delayed onset in 60%.)
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.