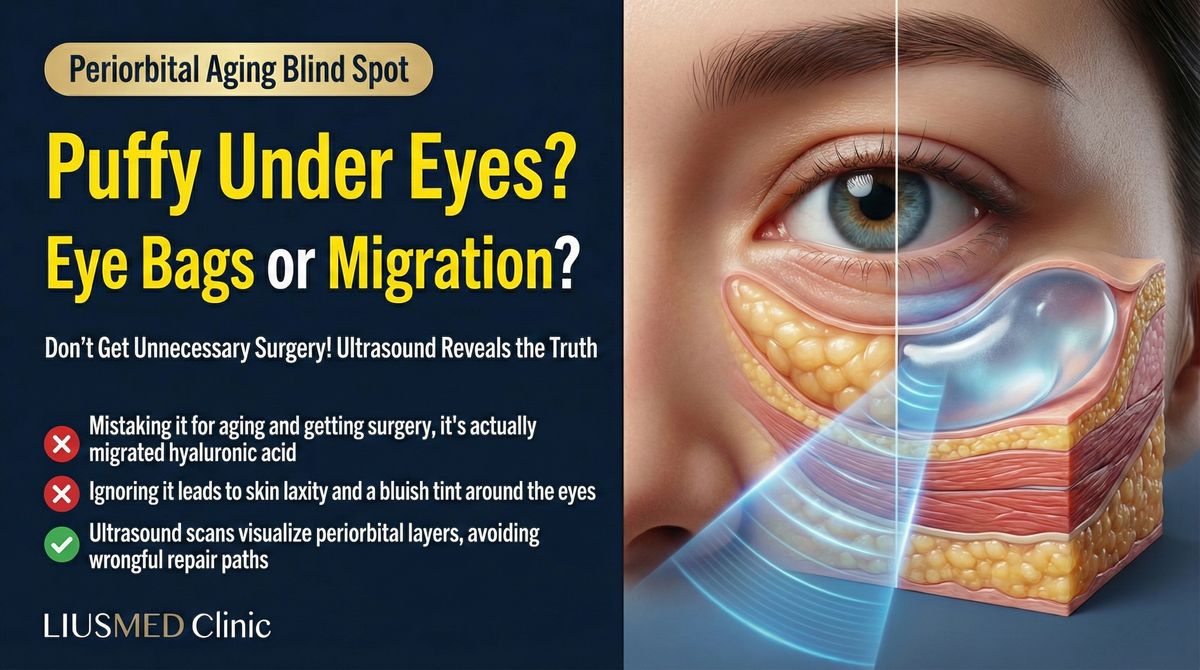
Why Do My Under-Eyes Look Blue After Filler?
"My doctor said the blue tint would fade, but it's been over a year and it's still there. I tried hyaluronidase twice and it barely changed." At FILLER REVISION, this is one of our most frequent consultations. The persistent bluish discoloration beneath the eyes after tear trough filler is most commonly caused by the Tyndall effect—a well-documented optical phenomenon that occurs when hyaluronic acid filler is placed too superficially in the delicate under-eye skin. In our experience, roughly half of Tyndall effect patients who reach us have already attempted dissolution elsewhere without satisfactory results.
This article explains what the Tyndall effect is, how to differentiate it from other under-eye complications, and what treatment options are available.
What Is the Tyndall Effect?
The Optical Phenomenon
The Tyndall effect is a light-scattering phenomenon that occurs when particles suspended in a medium scatter shorter wavelengths of light (blue light) more than longer wavelengths. In the context of dermal fillers:
- Hyaluronic acid is a clear, gel-like substance
- When placed too close to the skin surface, it scatters incoming light
- Blue wavelengths are preferentially scattered, creating a visible bluish tint
- The effect is more pronounced in areas with thin, translucent skin—like the under-eyes
← Swipe to see more →
| Factor | Impact on Tyndall Effect |
|---|---|
| Injection depth | Shallower placement = more visible blue tint |
| Filler volume | More volume = more pronounced effect |
| Skin thickness | Thinner skin = easier to see through |
| HA (Hyaluronic Acid) particle size | Larger particles scatter more light |
| Skin tone | More visible in lighter skin tones |
Why the Under-Eye Area Is Particularly Vulnerable
The periorbital region has several characteristics that make it prone to the Tyndall effect:
- Extremely thin skin: The under-eye skin is only 0.5mm thick—the thinnest on the face
- Minimal subcutaneous fat: Less tissue between filler and skin surface
- Rich vascular network: Adds complexity to the visual appearance
- Limited tissue layers: Fewer anatomical planes for filler placement
- High visibility: Any imperfection is immediately noticeable
Key Insight: At FILLER REVISION, we see this pattern regularly — the Tyndall effect is not an allergic reaction or infection. It is a purely optical phenomenon caused by filler placement, and it will not resolve on its own as long as the filler remains in place. Patients are often reassured it will fade, but without intervention, it persists indefinitely.
Is It the Tyndall Effect or Something Else?
Differential Diagnosis
Not all blue or purple discoloration under the eyes is caused by the Tyndall effect. A proper assessment must rule out other conditions:
← Swipe to see more →
| Condition | Key Features | How to Differentiate |
|---|---|---|
| Tyndall effect | Bluish tint, worsened in certain light, appeared after filler | Pressing the skin may reveal underlying blue gel |
| Vascular dark circles | Purple-red tone, present before filler | Improves when skin is stretched |
| Bruising | Appeared shortly after injection, yellow-green evolution | Resolves within 2–3 weeks |
| Filler migration | Puffiness or irregularity extending beyond injection site | Palpable material in unexpected areas |
| Venous congestion | Dark circles that worsen with fatigue or allergies | Bilateral, fluctuates with lifestyle |
| Malar edema | Festoon-like swelling on the cheekbone | Worsens with salt intake, morning puffiness |
The Ultrasound (Ultrasonography) Advantage
High-frequency ultrasound provides definitive answers:
- Visualizes filler location: Confirms whether HA is placed too superficially
- Measures depth: Quantifies the distance between filler and skin surface
- Identifies volume: Estimates how much filler is present
- Rules out complications: Detects vascular compromise or abscess formation
- Guides treatment: Determines whether dissolution or extraction is more appropriate
Dr. Liu explains: "Many patients are told their blue tint is just bruising that will fade. If the discoloration persists beyond three weeks after injection, it is almost certainly the Tyndall effect and will not improve without treatment."
What Happens When Tear Trough Filler Goes Wrong?
Beyond the Tyndall Effect
Superficially placed tear trough filler can cause additional problems:
← Swipe to see more →
| Complication | Description |
|---|---|
| Chronic puffiness | HA absorbs water, creating persistent swelling |
| Irregularity | Visible lumps or ridges beneath thin skin |
| Festooning | Fluid accumulation creating bag-like swelling |
| Asymmetry | Uneven appearance between the two sides |
| Overcorrection | Overfilled appearance that looks unnatural |
These complications often coexist with the Tyndall effect, and they share the same root cause: filler placed in the wrong tissue plane or in excessive volume.
Why Tear Trough Injection Is High-Risk
The tear trough is considered one of the most technically demanding areas for filler injection:
- The margin of error for depth is less than 1mm
- Individual anatomy varies significantly
- Filler behavior in this area is unpredictable
- Overcorrection is common because under-correction looks like a failed result
- The area is unforgiving—any imperfection is visible in every mirror check
Treatment Options for Tyndall Effect
Option 1: Hyaluronidase Dissolution
For recent HA filler placement (less than 12 months), hyaluronidase injection is often the first-line treatment:
← Swipe to see more →
| Advantage | Limitation |
|---|---|
| Non-surgical | May require multiple sessions |
| Quick procedure | Can dissolve native HA (temporary hollowing) |
| Minimal downtime | Difficult to control precisely in thin-skinned areas |
| Cost-effective | Less effective on encapsulated or old filler |
Important considerations:
- Hyaluronidase does not distinguish between injected HA and the body's natural HA
- The under-eye area may appear temporarily more hollow after dissolution
- Results vary based on filler brand, cross-linking density, and time since injection
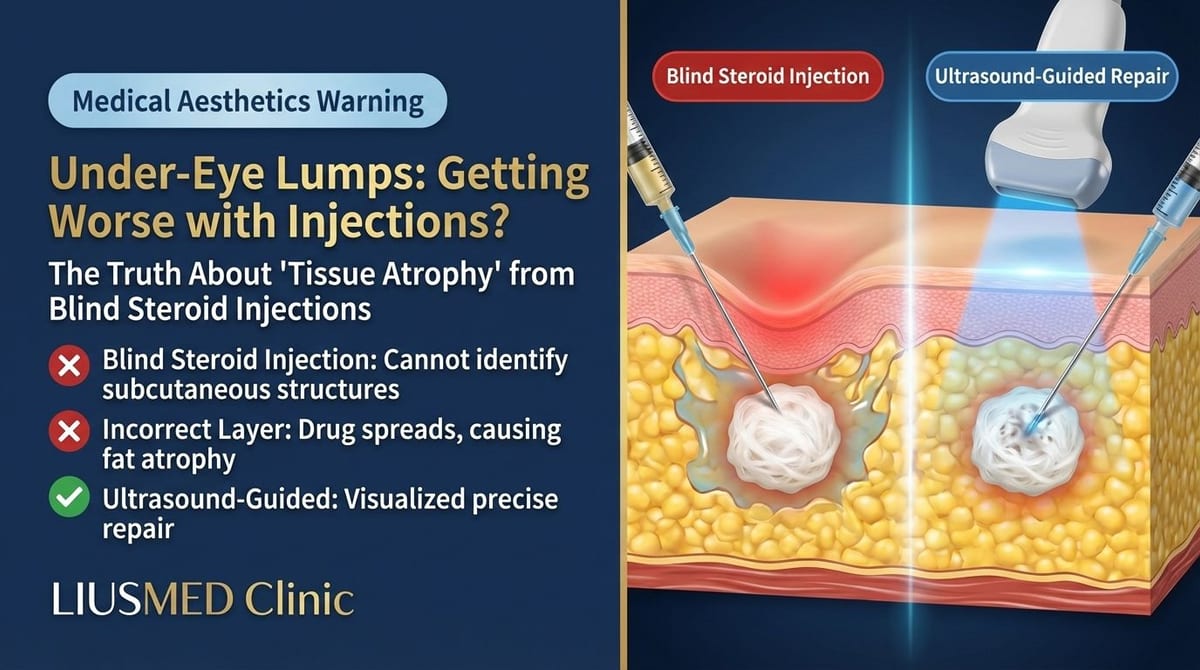
Option 2: Ultrasound-Guided Extraction
For filler that has been present for over a year, has become partially encapsulated, or has failed to respond to hyaluronidase, physical extraction under ultrasound guidance offers a more definitive solution:
- Ultrasound identifies the exact location and volume of remaining filler
- Pinhole incision (1-2mm) in a concealed location
- Direct visualization allows selective removal of filler material
- Real-time confirmation that the Tyndall-causing material has been removed
- Tissue preservation ensures no unnecessary damage to the delicate periorbital area
Which Treatment Is Right for Me?
← Swipe to see more →
| Factor | Hyaluronidase | Extraction |
|---|---|---|
| Filler age | < 12 months | > 12 months or encapsulated |
| Previous dissolution attempts | First attempt | Failed dissolution |
| Filler volume | Small amounts | Larger or migrated deposits |
| Patient preference | Non-surgical approach | Definitive one-time solution |
| Complexity | Straightforward cases | Multiple complications present |
When Dissolution Alone Isn't Enough: The FILLER REVISION Approach
Many patients arrive at FILLER REVISION after one or more rounds of hyaluronidase that failed to fully resolve their Tyndall effect. The reason dissolution alone often falls short in the under-eye area is the unique anatomy: the periorbital skin is the thinnest on the face, and filler deposits here become partially encapsulated or lodged in tissue planes where enzymatic access is limited. At FILLER REVISION, we use high-frequency ultrasound to precisely map residual filler deposits, then perform targeted pinhole extraction of material that hyaluronidase cannot reach. This approach addresses the root cause — physically removing the superficially placed filler — rather than relying solely on enzymatic breakdown that may incompletely dissolve the offending material.
Recovery and Expected Results
After Hyaluronidase
- Swelling for 24–48 hours
- Results visible within 3–7 days
- May need repeat treatment if filler persists
- Temporary under-eye hollowing is common
After Extraction
- Mild swelling for 3–5 days
- Bruising possible for 7–10 days
- Blue tint resolves immediately upon filler removal
- Final contour assessment at 4–8 weeks
Dr. Liu's approach: "For Tyndall effect cases, I always start with a thorough ultrasound assessment. This tells me exactly how much filler is there, where it sits, and whether dissolution or extraction will give the best result. There is no one-size-fits-all solution for under-eye filler complications."
Prevention: What Went Wrong and How to Avoid It
Key Factors in Safe Tear Trough Injection
← Swipe to see more →
| Principle | Explanation |
|---|---|
| Proper depth | Filler must be placed at the sub-orbicularis oculi fat (SOOF) or periosteal level |
| Conservative volume | Start with less (0.3–0.5ml per side), assess, then add if needed |
| Appropriate product | Low-viscosity, small-particle HA designed for delicate areas |
| Cannula technique | Blunt cannula reduces risk of superficial placement and bruising |
| Patient selection | Not every patient is a good candidate for tear trough filler |
Frequently Asked Questions
Will the Tyndall effect go away on its own?
No. Unlike bruising, the Tyndall effect persists as long as the superficially placed filler remains. HA fillers can last 12–18 months or longer in the under-eye area, where metabolic activity is low. Treatment is required for resolution.
Can I have new filler placed after treatment?
Yes, but it is advisable to wait at least 3–6 months after the Tyndall-causing filler is removed. If re-injection is considered, it should be performed by a practitioner experienced in deep-plane tear trough techniques.
Is the Tyndall effect dangerous?
It is not medically dangerous, but it is aesthetically significant and psychologically distressing for many patients. In rare cases, superficial filler placement can also contribute to chronic swelling and lymphatic obstruction.
Get Your Under-Eyes Evaluated
If you've already tried treatment for Tyndall effect or under-eye filler complications without success, FILLER REVISION specializes in exactly these cases. Our ultrasound-guided approach pinpoints residual filler that dissolution alone cannot reach, providing a definitive path to resolution.
About the Author
Dr. Ta-Ju Liu
- Current Position: Director, Liusmed Clinic
- Specialties: Minimally invasive surgery (lipoma, cyst), hyperhidrosis surgery, thread lifting, filler complication repair
- Experience:
- 15+ years of clinical minimally invasive surgery experience
- Over 10,000 successful minimally invasive cases
- Board-certified dermatologist
- Philosophy: "The under-eye area demands the highest precision. When filler complications occur here, accurate diagnosis with ultrasound is essential before any intervention."