
Fat Graft Complication Repair Complete Guide
"Fat Turned to Stone — Even Liposuction Can't Remove It"Other Doctors Gave Up? FILLER REVISION Takes Over From Here
"Three years ago I got fat grafting, and my forehead and temples became hard as stone. My original doctor said just suction it out again — it only made it worse, leaving craters. Steroids made it even more uneven." At FILLER REVISION, cases like this — made worse by previous attempts — account for over 70% of our consultations. FOS (pillow face), calcified lumps, under-eye fat granulomas — Dr. Liu's ultrasound-guided "Micro-Pinhole Extraction" precisely removes fibrotic fat masses through just 1-2mm micro-incisions, built for the cases others cannot solve.
Table of Contents
Are You Experiencing These Issues?
Fat graft complications are more common than many people realize. Here are the most frequent issues:
Common Fat Graft Complications
"Liposuction left craters, steroids caused deformity, laser caused hyperpigmentation" — at FILLER REVISION, we handle cases every day where other methods made things worse. The problem was never you — it was the wrong approach.
Pathological Mechanisms: Why Do Fat Grafts Go Wrong?
Although fat grafts use "your own" tissue, not all transplanted fat cells survive. Understanding the pathology is key to effective treatment.
Central Necrosis → Fibrous Encapsulation → Calcification
The Fate of Fat Masses
When the radius of a single-point fat injection exceeds 2 mm, the core of the fat bolus cannot receive sufficient oxygen diffusion or neovascular supply within the first 48 hours, resulting in central necrosis. Necrotic fat releases free fatty acids, triggering sterile inflammation — the immune system dispatches macrophages to form a dense, rigid fibrous capsule wall. This is why the lump feels as hard as a "stone." Over time, calcium deposits accumulate within the necrotic core, forming permanent calcified nodules that no lipolytic injection can dissolve.
FOS: Compartment Destruction & Expression Restriction
Chain Reaction of Excess Fat
In pursuit of volume, excessive fat is injected into both the superficial and deep fat compartments, destroying the face's precisely organized "retaining ligament" architecture. Fat overflows into layers where it shouldn't exist, compressing the mimetic muscles — when fat is inadvertently injected into the muscular layer or accumulates on top of expression muscles, muscular contraction meets mechanical resistance, producing the characteristic "plastic" appearance with every smile. More filling leads to more swelling, which leads to looking older — that is the essence of FOS.
Periorbital: Granuloma & Permanent Edema
The Truth Behind Under-Eye "Caterpillars"
The under-eye skin is approximately only 0.5 mm thick — the thinnest on the entire face. Necrotic fat cells after grafting trigger granulomatous reactions, forming visible "caterpillar"-like strip or granular bumps under directional lighting. Worse still, excessive fat masses compress the delicate periorbital lymphatic network, obstructing lymphatic drainage and causing chronic, non-resolving malar edema. This swelling will not resolve over time — it can only improve by physically removing the offending tissue.

Why Traditional Methods Fail: The Dead Ends of Conventional Repair
Repairing fat graft complications is far more difficult than conventional fillers because fat integrates tightly with native tissue and fibrosis is more severe. Here are the limitations of traditional methods:
Traditional Liposuction
Liposuction cannulas are designed to aspirate soft, mobile fat. Against dense fibrotic lumps, the cannula simply glides over the surface like sliding across a stone — unable to gain purchase. Forceful manipulation only damages the surrounding healthy tissue, creating surface irregularities and making the problem worse.
Steroid Injections
Killing one hundred enemies, wounding three thousand allies. Steroids cannot selectively target the lump — the typical outcome: the hard core persists while surrounding healthy fat atrophies, creating unsightly "volcanic crater" depressions. Completely ineffective against calcified lumps, and actually increases the complexity of subsequent repair.
Laser Lipolysis
Dissolving calcified deposits requires elevated laser energy. In thin-skinned areas like the forehead and periorbital region, this substantially increases the risk of thermal skin burns and nerve heat injury. Laser heat also cannot precisely distinguish fibrotic tissue from normal tissue, easily causing irreversible collateral damage.
Open Excision
Although the most thorough approach, making a 2-3 cm incision on the face and accepting a permanent scar is simply unacceptable for patients seeking aesthetic improvement. Extensive tissue dissection also risks nerve damage and tissue collapse, with significantly prolonged recovery.
Core Technology: Ultrasound-Guided Micro-Pinhole Extraction
Four-Step Precision Repair: From Localization to Aesthetic Reshaping
High-Frequency Ultrasound Guidance
Visualized Surgery
We refuse to operate blindly. Using high-resolution soft-tissue ultrasound, we perform a full-face tomographic scan before the procedure. This precisely maps the depth, nature (liquid oil cyst vs. calcified lump), and surrounding vascularity of each deposit. This "navigation map" is the cornerstone of surgical success — giving the surgeon a complete subcutaneous roadmap before any incision.
Precision Micro-Dissection
Separating Lesion from Normal Tissue
When working in high-risk zones such as the forehead (supratrochlear nerve territory) and periorbital region, safety is the paramount principle. Through a mere 1-2mm pinhole entry, specialized micro-instruments gently dissect the lump away from surrounding neurovascular structures, creating a safe buffer zone and preserving healthy tissue before proceeding.
Pinhole Micro-Fragmentation & Extraction
Breaking Down and Removing Piece by Piece
This is the technical heart of the procedure. We abandon the crude liposuction cannula in favor of microsurgical energy devices. Hardened calcified deposits are pulverized "in situ" beneath the skin — breaking the large "stone" into fine "sand" particles before precise aspiration, completely removing stubborn calcifications that even laser cannot eliminate. The entire process requires only a 1-2mm pinhole incision.
Subtractive Aesthetics & Tissue Repositioning
Not Just Removal, But Restoration
To address skin laxity from FOS correction, we sculpt the subcutaneous space and apply "skin re-adherence techniques," allowing the skin to re-adhere naturally to the deeper tissue framework, restoring the face's original bony contours. The core philosophy of "subtractive aesthetics": removing what's excess requires more skill than adding more — it's not just removal, but restoration.
FAQ
Can calcified fat graft lumps from years ago still be treated?
Yes. Regardless of how much time has passed, as long as the lump still exists and causes problems, we can precisely treat it with ultrasound-guided minimally invasive methods. Even stone-hard calcified lumps can be safely removed through our pinhole micro-fragmentation extraction technique.
Will my face look sunken after fat removal?
This is the most common concern, but the answer is actually the opposite. Overfilling or excess fat makes you "look older." After precisely removing the excess and displaced fat, facial contours actually return to a younger, more natural state. We apply "subtractive aesthetics" philosophy combined with tissue repositioning techniques to ensure smooth, natural post-operative contours.
Can under-eye fat granulomas (caterpillars) be treated?
Yes. Under-eye fat granulomas are among the trickiest complications of fat grafting. We use ultrasound to precisely locate the granuloma's layer and extent, then carefully extract through a micro-pinhole approach while avoiding the delicate periorbital neurovascular network. Recovery takes about 1-2 weeks, restoring smooth, natural under-eye contours.
Is general anesthesia required? How long is recovery?
Most cases require only local anesthesia with no hospitalization needed. The wound is just 1-2mm pinhole-sized. There may be mild swelling and bruising post-op, typically recovering for normal social activities within 1-2 weeks. Recovery time is significantly shorter compared to traditional open surgery.
Why aren't steroids recommended for fat graft lumps?
Steroids indiscriminately dissolve normal fat, creating "crater" depressions that are even harder to repair. Moreover, steroids are completely ineffective against calcified or fibrotic masses. Clinically, patients who received steroid injections often develop more severe surface irregularities, actually increasing the complexity of subsequent repair.
My fat graft lump has been there for five years — is it too late?
It's not too late, but it will be more challenging. Fat masses over five years old are typically fully fibrotic or even calcified, extremely hard, and more adherent to surrounding tissues. This increases surgical difficulty, which is exactly why a secondary revision specialist like FILLER REVISION is needed. Ultrasound (Ultrasonography) guidance precisely maps the mass boundaries and adhesion extent, allowing layer-by-layer dissection through a micro-pinhole approach. Our longest case was a calcified mass over ten years post-injection — it was still successfully removed intact. The sooner you act the easier it is, but "too late" does not mean "impossible."
How is pricing determined?
Fat graft repair is a highly customized medical procedure. Cost depends on the number of fat masses, their depth and location, degree of fibrosis/calcification, and severity. Pricing requires the doctor's hands-on examination and ultrasound assessment. We insist on providing only necessary treatment without wasting patients' money.
I had a failed fat graft revision at another clinic. Can you still help?
Yes. A significant proportion of our patients come to us seeking a second opinion after unsuccessful liposuction, steroid injections, or laser lipolysis at other clinics. A previous failed attempt does not mean the problem is irreparable — it means a more precise technique is needed. Our ultrasound-guided micro-pinhole extraction can navigate around scar adhesions from prior surgeries, precisely locating and removing residual fibrotic or calcified masses. We perform a full reassessment for every case, unconstrained by previous treatments.
Repair Process
Precise Assessment × Micro Repair × Complete Follow-up
Consultation
Understanding your situation, fat graft history, and expectations with hands-on examination and ultrasound assessment
Treatment Planning
Developing personalized plan and pricing based on assessment
Micro Repair
Precise ultrasound-guided minimally invasive repair, wound only 1-2mm
Follow-up Care
7-14 day post-op follow-up to ensure smooth recovery
Dr. Ta-Ju Liu
Director, Liusmed Clinic
Specialties
Credentials
- 20+ years clinical minimally invasive surgery experience
- One of the few specialists in Taiwan focused on "fat graft complication repair"
- Developed ultrasound-guided micro fat repair techniques
"Fat graft revision patients who walk into FILLER REVISION have typically seen three doctors already. They're not here for comfort — they're here for someone who can actually fix the problem. That's why I come to work every day."
Other Repair Services
Real medicine means standing by patients when problems arise.
We hope Liusmed can be your "rescue station."
References
- Coleman SR, Saboeiro AP. Fat grafting to the breast revisited: safety and efficacy. Plast Reconstr Surg. 2007;119(3):775-785.
- Yoshimura K, et al. Complications and patient satisfaction after facial fat injection. Plast Reconstr Surg. 2008;121(3):e219-e228.
- Khouri RK, et al. Brava and autologous fat transfer is a safe and effective breast augmentation alternative. Plast Reconstr Surg. 2012;129(5):1071-1079.
The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
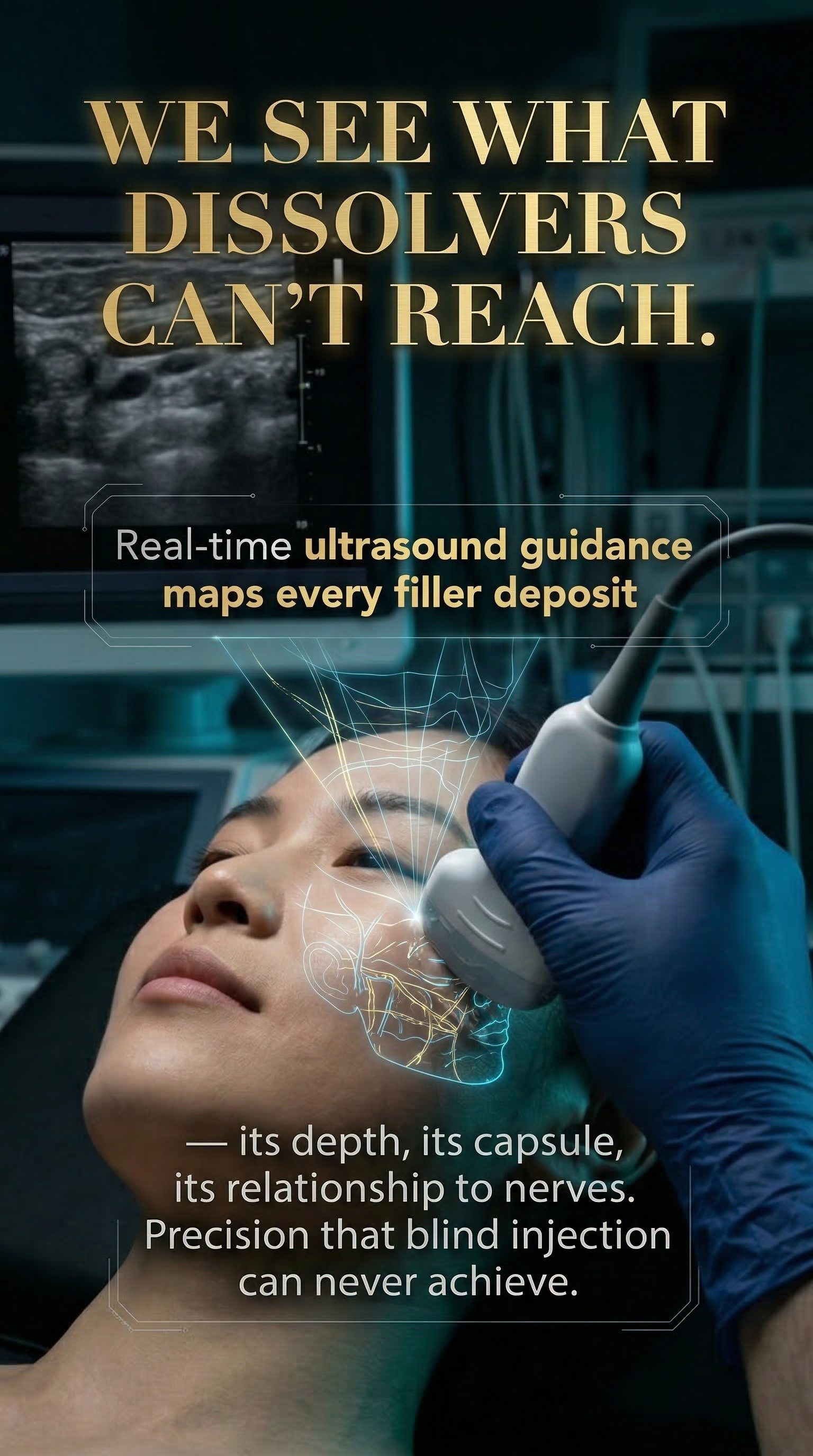
We see what dissolvers can't reach.
Real-time ultrasound guidance maps every filler deposit — its depth, its capsule, its relationship to nerves.
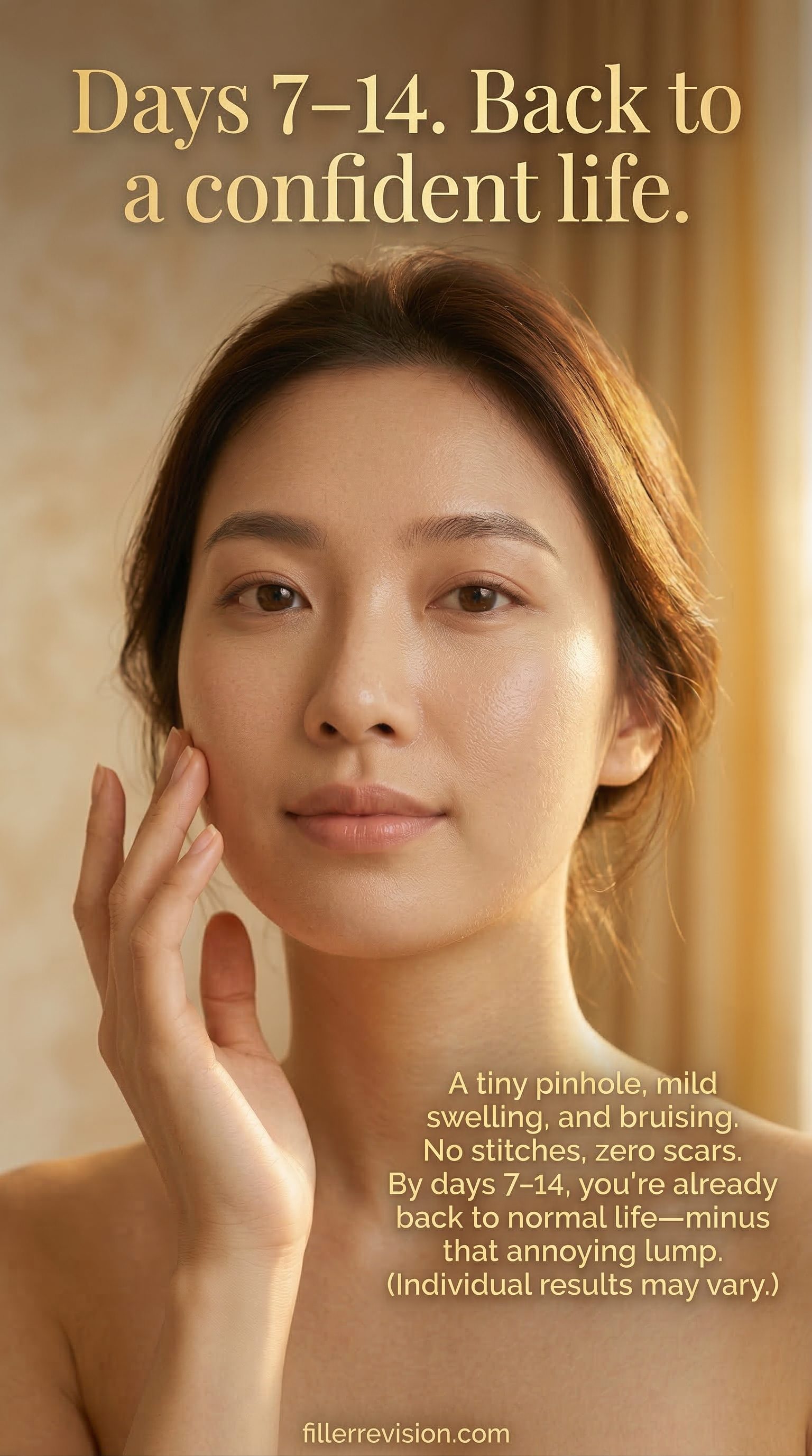
Days 7–14. Back to a confident life.
A tiny pinhole, mild swelling, and bruising. No stitches, zero scars. By days 7–14, you're already back to normal life — minus that annoying lump.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
"Suctioned, Injected, Lasered — Nothing Worked" — FILLER REVISION Finishes What Others Couldn't
Over 70% of our fat revision patients found us after failing elsewhere — their story might be exactly like yours
Every day a calcified fat mass remains, the fibrous capsule grows thicker. Book a FILLER REVISION fat revision evaluation now — let us see what we can still do for you
Book Consultation