
Foreign Body Granulomas
"Every time I catch a cold, the lump flares up. I've been on steroids four times this year and my doctor just keeps prescribing more." At FILLER REVISION, granuloma patients arrive after the longest suffering — months or years trapped in the flare-suppress-repeat cycle. A foreign body granuloma is an organized chronic inflammatory reaction where the immune system forms a dense capsule of macrophages, giant cells, and fibrous tissue around filler material it cannot break down. They can develop with any filler type—including HA, biostimulators, fat, and permanent fillers—and may appear months to years after injection. The reason steroids never provide lasting relief is that they suppress the immune response without removing the foreign body driving it.
Common Symptoms
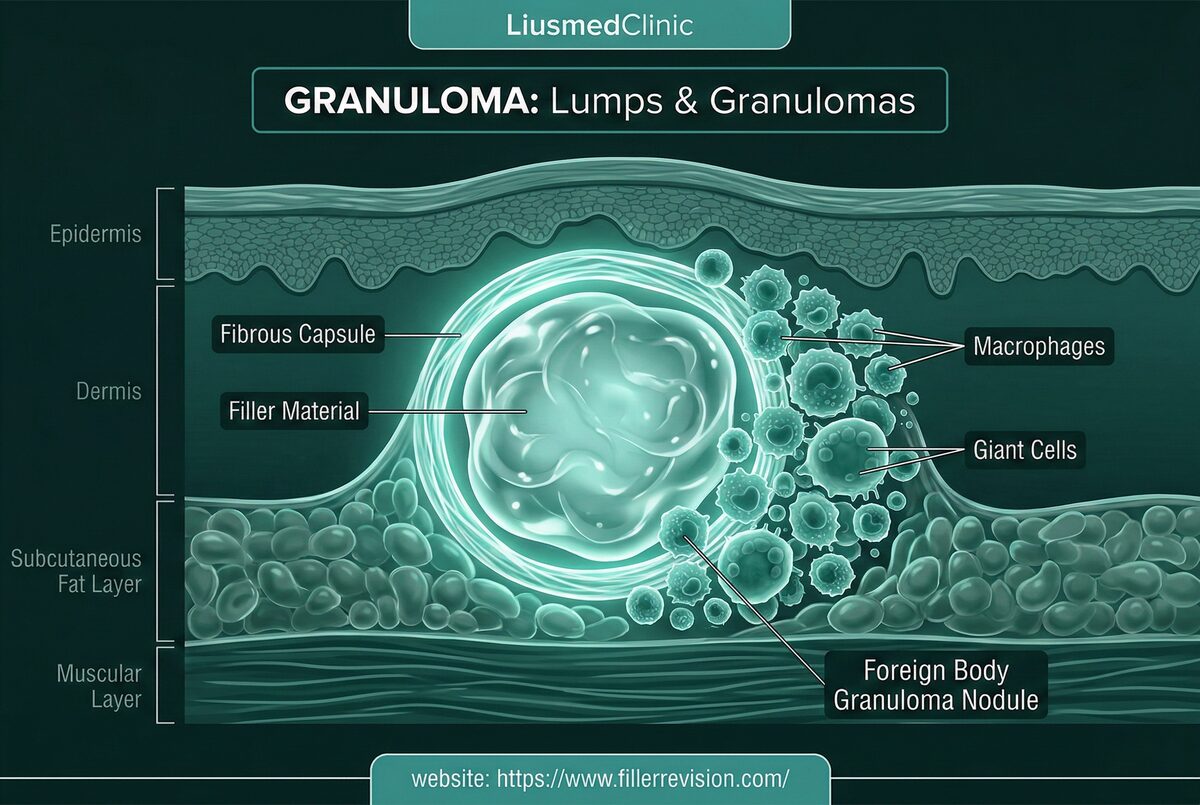
The Foreign Body Immune Cascade
If you've been prescribed round after round of steroids for a granuloma that keeps coming back, the frustration is understandable — but the explanation is simple. Your immune system isn't malfunctioning; it's responding correctly to a foreign body that's still inside. The mechanism explains why this cycle never ends. Macrophages engulf filler particles but cannot break them down, fusing into multinucleated giant cells. These cells release inflammatory cytokines that recruit more immune cells, creating an escalating cycle of inflammation and fibrosis. The resulting granuloma has a characteristic layered architecture: a central core of filler material surrounded by giant cells, then a ring of inflammatory infiltrate, encased in a dense fibrous capsule. This process can be triggered months or years after injection by immune system activation—explaining why granulomas often appear after unrelated illness, vaccination, dental work, or periods of significant stress.
Why Traditional Treatments Fail
Limitations of Immunosuppressive Treatment
The standard treatment—intralesional corticosteroid injection—suppresses the inflammatory component and can temporarily shrink the granuloma. However, it does not remove the foreign body trigger at the core. Once steroid effects dissipate, the immune system re-engages and the granuloma recurs, often with increased fibrosis from each inflammatory cycle. Repeated steroid injections cause cumulative tissue damage: fat atrophy creating visible skin depressions, dermal thinning, telangiectasia, and hypopigmentation that can be more disfiguring than the original granuloma. Other immunomodulatory agents carry similar limitations—they manage symptoms without addressing the root cause. Only physical removal of the foreign body source provides definitive resolution.
“Granuloma patients at FILLER REVISION have often suffered the longest of anyone I see — some for years, trapped in steroid cycles they know aren't working but have no alternative to. The turning point is always the same: when I show them the ultrasound image of the foreign body still sitting inside, surrounded by their own immune cells trying to destroy it. They instantly understand that no amount of medication will make this go away. Only removing the source ends the war.”
Dr. LiuSource Elimination, Not Symptom Suppression
Ultrasound-Guided Pinhole Micro-Extraction
A granuloma is not a disease — it's the immune system doing exactly what it's supposed to do: attacking a foreign body it cannot break down. Suppressing the immune response with steroids is fighting the wrong enemy. The only definitive solution is removing what the immune system is reacting to.
Steroids Fight the Wrong Battle
At FILLER REVISION, granuloma patients arrive after months — sometimes years — of steroid cycles prescribed as if their immune system is the problem. It's not. Their immune system is doing exactly what it should: attacking a foreign body it can't break down.
Every Failed Steroid Cycle Adds Scar Tissue
The suppress-flare-suppress pattern doesn't just fail to cure — it actively makes revision harder. Each cycle deposits more fibrosis around the foreign body, thickening the capsule and complicating the extraction that was always the definitive answer.
Remove the Trigger, End the War Permanently
Extracting the foreign body and its inflammatory capsule eliminates the antigenic stimulus your immune system has been fighting. No more cyclical flares, no more steroid side effects, no more scheduling your life around unpredictable swelling episodes.
Complete Capsule Extraction
We target the root cause: complete removal of the foreign body and its surrounding inflammatory capsule. Using ultrasound to precisely map the granuloma borders—including any satellite lesions—we extract the entire capsule intact through a minimal incision. This removes both the filler trigger and the organized immune tissue, eliminating the source of chronic inflammation rather than merely suppressing symptoms.
Border Mapping
Local Anesthesia
Capsule Extraction
Anti-inflammatory Protocol
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
No, foreign body granulomas are benign inflammatory reactions—not malignant tumors. However, they can be disfiguring, painful, and progressive. In rare cases where the clinical presentation is atypical, we may recommend fine-needle biopsy to confirm the diagnosis before treatment. Ultrasound characteristics of granulomas are distinct from malignant masses, providing additional diagnostic confidence.
There may be some volume loss where the granuloma was, as the inflammatory mass itself had been occupying space. In most cases, the surrounding tissue remodels naturally over 4-8 weeks. For larger granulomas where significant volume loss is expected, we can plan restorative treatment with fat grafting or safe fillers after complete healing and confirmation that the inflammation has resolved.
Granulomas can appear anywhere from 6 months to several years after injection. They represent a delayed hypersensitivity reaction, not an immediate complication. The trigger is often an immune activation event—illness, stress, vaccination, or dental procedures—that tips the balance from immune tolerance to active rejection of the foreign material.
Steroids suppress the inflammatory component but cannot dissolve or remove the foreign body at the core. Recurrence is the rule once steroids are discontinued. Each cycle of inflammation and steroid suppression adds more fibrotic tissue, making the granuloma progressively harder to treat. Complete physical removal of the foreign body source is the only approach that provides definitive resolution.
Immune system activation is the common trigger. Any event that stimulates immune surveillance—viral illness, bacterial infection, vaccination, dental procedures, significant psychological stress, or even hormonal changes—can reactivate the inflammatory cells surrounding the foreign body. This explains the characteristic cyclical pattern: the granuloma appears stable for months, then suddenly swells and becomes painful.
In most cases, ultrasound imaging provides sufficient diagnostic information—granulomas have characteristic echographic features that distinguish them from other masses. However, if the clinical presentation is atypical, if the mass is in an unusual location, or if there is any diagnostic uncertainty, a fine-needle biopsy is recommended before definitive treatment to ensure accurate diagnosis.
Granulomas don't metastasize like cancer, but they can extend along tissue planes or develop at multiple sites where filler was deposited. If the immune trigger event is systemic (like a viral illness), multiple previously-stable filler sites may develop granulomatous reactions simultaneously. This is why comprehensive ultrasound scanning of all treated areas is important.
Prolonged steroid use carries significant cumulative risks: fat atrophy (creating visible depressions), skin thinning, telangiectasia, and hypopigmentation. If your granuloma has not resolved after 3-4 steroid cycles, it is unlikely to resolve with continued injections — the foreign body trigger remains. At this point, extraction should be seriously considered to end both the granuloma and the steroid side effects.
Yes. Delayed granuloma formation is well-documented and characteristic of filler complications. The foreign body may coexist peacefully with the immune system for months or years until an activation event — illness, vaccination, dental work, significant stress — tips the balance from tolerance to active rejection. The timing of onset does not diminish the causal relationship.
Yes — ultrasound imaging definitively shows the foreign body, its capsule, and the surrounding inflammatory tissue. At FILLER REVISION, we see granulomas from every filler type: HA, biostimulators, fat, permanent fillers. The ultrasound appearance tells us the material type, the capsule thickness, and the optimal extraction approach — information that clinical examination alone cannot provide.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Lemperle G, et al. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009;123(6):1842-1863.
- Alijotas-Reig J, et al. Late-onset inflammatory adverse reactions related to soft tissue filler injections. Clin Rev Allergy Immunol. 2013;45(1):97-108.
- Requena L, et al. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1-34.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.