
Fat Grafting Lumps & Calcification
"My surgeon says it's just swelling — but it's been eight months and the lumps are getting harder, not softer." At FILLER REVISION, fat grafting patients arrive after months of being told to wait — only to discover that what they're feeling isn't swelling at all. When injected fat cells fail to establish blood supply, they undergo necrosis — cell death that creates oil cysts, fibrous lumps, or calcified nodules that the body cannot reprocess. Studies report palpable lump rates of 5-15% following facial fat grafting. The frustration is compounded because these complications involve your own tissue, making them nearly impossible to distinguish from normal anatomy without ultrasound — and because the advice to "just wait" allows oil cysts to calcify into rock-hard masses that become progressively harder to treat.
Common Symptoms
Fat Necrosis & Calcification Cascade
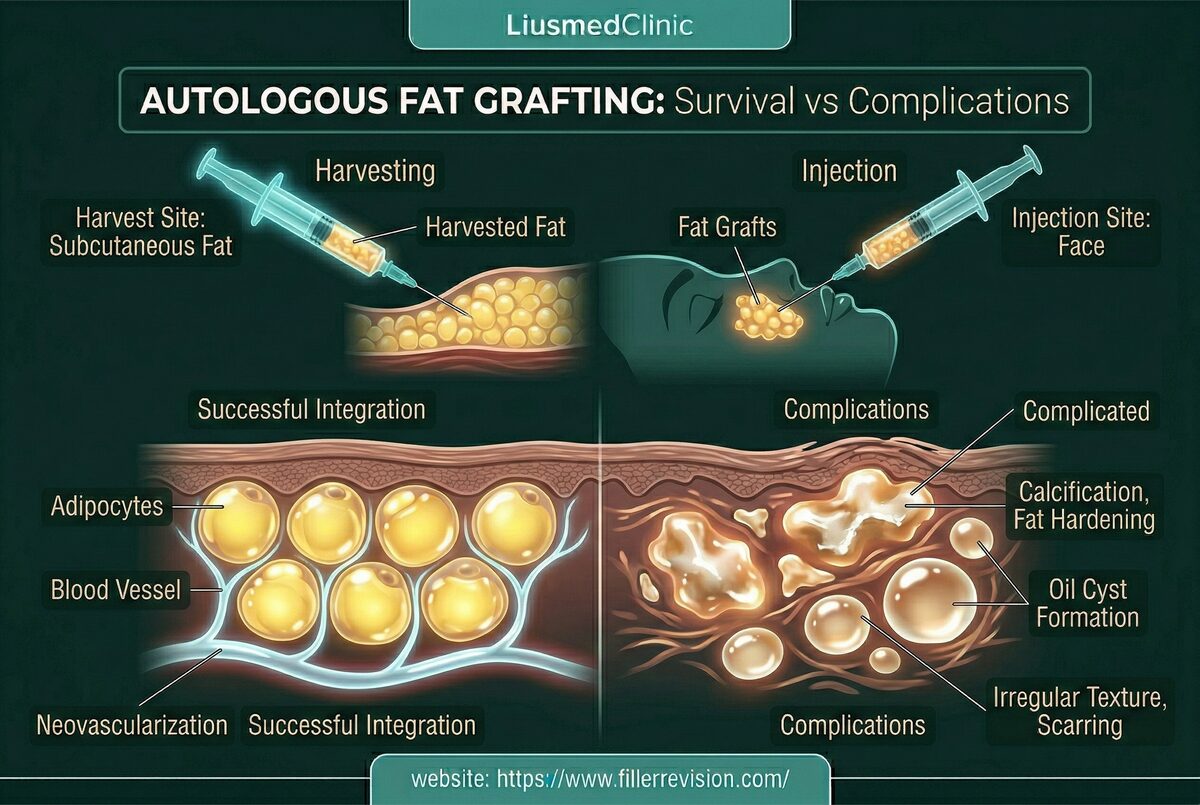
By the time fat grafting patients reach FILLER REVISION, they've typically waited 6-12 months on their surgeon's assurance that the lumps would soften. They haven't — and they won't. Here's the biology that explains why waiting was never going to work. Fat survival after grafting depends on rapid revascularization—the transferred cells must establish a blood supply within 48-72 hours or they die. Factors that impede this process include over-injection of large boluses (exceeding the tissue's ability to nourish), placement in poorly vascularized areas, rough handling of harvested fat, and individual patient healing response. Dead fat cells rupture, releasing their lipid contents into the surrounding tissue. The body attempts to contain this oil through encapsulation—forming oil cysts. Over months, inflammatory mediators and calcium deposition convert some of these cysts into calcified nodules—rock-hard masses that are indistinguishable from pathological calcifications on imaging and frequently trigger unnecessary cancer workups.
Why Traditional Treatments Fail
Risks of Conventional Surgical Approach
Traditional surgical excision of fat lumps requires incisions that leave visible scars on the face. Conventional liposuction cannulas are designed for body contouring and are too large and aggressive for delicate facial structures—risking nerve damage, uncontrolled volume loss, and contour irregularities (dents). Steroid injections can reduce inflammation around oil cysts but cannot dissolve calcified tissue and risk causing fat atrophy in surrounding healthy fat. Observation is often recommended but is inadequate for symptomatic lesions—calcified nodules will not resolve spontaneously and oil cysts rarely fully absorb.
“At FILLER REVISION, fat grafting patients arrive carrying the same story: their surgeon told them to wait, their surgeon said it was normal swelling, and months later the lumps are harder than ever. The moment I put the ultrasound probe on and show them exactly what's inside — oil cyst here, calcification there, healthy fat everywhere else — they understand why 'just waiting' was never going to work. A lump is not a diagnosis, and the treatment that resolves an oil cyst does nothing for a calcification.”
Dr. LiuFour Pathologies, Four Different Treatments
Ultrasound-Guided Pinhole Micro-Extraction
The critical insight with fat grafting complications is that 'a lump' is not a diagnosis. Every palpable abnormality falls into one of four distinct categories — viable fat, oil cyst, fibrous mass, or calcification — and each requires a completely different treatment. Treating all lumps the same way is the most common clinical error.
You Were Told to Wait — That Window Is Closed
FILLER REVISION patients have typically waited 6-12 months on their surgeon's advice before seeking help. During that time, oil cysts didn't absorb and soft lumps calcified into rock-hard nodules. Ultrasound classification tells you exactly what's inside — and confirms what waiting already proved.
Four Different Problems Need Four Different Solutions
Oil cysts need drainage, calcifications need fragmentation, fibrous masses need dissection, and healthy fat needs protecting. The single most common error we correct is one-size-fits-all treatment of fat grafting complications — because the approach that works for one pathology fails completely for another.
Revision Means Precision, Not Liposuction
The surviving fat that established blood supply is stable, natural, and irreplaceable. At FILLER REVISION, extraction targets only the dead tissue with ultrasound precision — not blind liposuction that removes healthy and necrotic fat alike.
Ultrasound-Guided Aspiration & Extraction
Using ultrasound, we first distinguish between viable fat, oil cysts, fibrous lumps, and calcified nodules—each requiring a different treatment approach. Oil cysts are drained via fine-needle aspiration. Calcified masses are mechanically broken down and extracted through micro-cannulas. Fibrous lumps are dissected and aspirated. Throughout, we preserve all healthy surrounding fat to maintain natural facial volume and contours.
Diagnostic Ultrasound Classification
Cyst Drainage
Calcification Breakdown
Micro-Cannula Extraction
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
We only remove the defective tissue—necrotic fat, oil cysts, and calcifications. Healthy surviving fat is preserved. The volume occupied by necrotic material was not providing useful aesthetic volume anyway (it was creating distortion), so most patients see improved contours rather than volume loss.
Yes, once necrotic tissue is removed, it does not grow back. The healthy fat that survived the original grafting procedure remains stable long-term. New complications would only arise from additional fat grafting procedures.
Lumps form when injected fat cells cannot establish blood supply quickly enough and undergo necrosis. Common contributing factors include injection of large boluses exceeding the tissue's vascular capacity, placement in poorly vascularized planes, rough fat processing, and individual patient healing factors. Even with optimal technique, some degree of fat necrosis is expected—clinically significant lumps occur in 5-15% of cases.
Yes, most facial fat calcifications can be treated with ultrasound-guided micro-cannula extraction. We mechanically break down the calcified shell and aspirate the contents through a needle-sized entry point. Only very large or deeply embedded calcifications adherent to periosteum may require a small incision approach.
Oil cysts typically form within 1-3 months as necrotic fat liquefies. Calcifications develop later—usually 6-12 months—as the body deposits calcium around dead tissue. Some calcifications continue to enlarge and harden over 1-2 years. Early ultrasound detection allows treatment before calcification becomes extensive.
Minor contour irregularity is possible for larger lumps, but the surrounding healthy fat typically remodels well over 4-8 weeks. Our technique preserves all viable fat, minimizing contour impact. For significant volume loss, corrective fat grafting can be performed after complete healing.
Fat necrosis calcifications in the face can appear alarming on imaging and may trigger concern. They are benign, but we recommend ultrasound evaluation to characterize the mass and distinguish it from other pathology. Once confirmed as fat necrosis calcification, treatment is for cosmetic and comfort reasons rather than medical urgency.
Some firmness in the first 2-3 months after fat grafting is part of normal healing. However, if palpable lumps persist beyond 6 months, are growing harder, or cause visible asymmetry, they are unlikely to resolve spontaneously. Oil cysts don't absorb, and calcifications only harden further with time. A second opinion with ultrasound assessment can determine whether you're dealing with normal healing or complications that need intervention.
Adding more fat over existing necrotic tissue, oil cysts, or calcifications is counterproductive — the new fat faces the same vascularization challenges in tissue already compromised by the failed graft. At FILLER REVISION, we always classify and treat the existing complications first. Once the necrotic material is removed and healing is complete, corrective fat grafting in healthy tissue can be considered if needed.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.