That Hard Ridge Along Your Smile Line—Should You Worry?
"I can feel a hard ridge along my smile line that wasn't there before. I tried dissolving it, but the lump stayed while the fold got deeper." At FILLER REVISION, nasolabial fold lumps are one of our most common consultations. Patients arrive after dissolution attempts that reduced overall volume in the fold — making it appear deeper — while leaving the actual lump untouched because it had already encapsulated. Understanding whether a palpable finding is normal filler texture or a true complication is the essential first step, and it requires ultrasound, not guesswork.
Let's break this down systematically.
Classifying Nasolabial Fold Lumps
Not Every "Palpable" Finding Is a Problem
← Swipe to see more →
| Type | What It Feels Like | Visible Change | Action Needed |
|---|---|---|---|
| Normal filler texture | Soft, diffuse, compressible with finger pressure | No visible abnormality | None |
| Filler aggregation | More defined cord or beaded shape | May or may not be visible | Case-dependent |
| Fibrous encapsulation | Hard cord, sharp borders, non-compressible | Possible subtle ridge | Recommended |
| Filler displacement | Mass palpable in unexpected location | Poor fold correction; new bulge nearby | Recommended |
| Inflammation/granuloma | Hard, tender, possibly red or swollen | Obvious bump, skin discoloration | Required |
Key Insight: At FILLER REVISION, we see this pattern regularly — because the nasolabial fold is a linear structure, filler injected along it is more likely to be palpable than in other facial areas. The question is not whether you can feel it, but what it feels like — its consistency, stability, and whether it's causing any problem. Ultrasound (Ultrasonography) provides the definitive answer.
Why Nasolabial Fold Lumps Resist Dissolution More Than Other Areas
Patients often ask the same question: "My doctor used the same hyaluronidase dose that worked for my cheek lump — why didn't it work on my smile line?" The nasolabial fold has three anatomical features that make encapsulated lumps especially resistant to enzymatic dissolution:
- Linear, confined tissue channel. Unlike the cheek or temple — where filler can spread three-dimensionally — the nasolabial fold sits along a fixed crease bounded by superficial musculoaponeurotic system (SMAS) fibers and the levator labii muscle. Filler injected here has nowhere to disperse, so it concentrates into cord-like deposits that the body walls off into a fibrous capsule much faster than in open tissue planes.
- High mechanical stress from facial expression. Every smile, every word you speak pulls and compresses filler along the fold. This repeated mechanical irritation accelerates fibroblast activation and capsule thickening — research suggests the encapsulation timeline at the nasolabial fold can be as short as 3–6 months, versus 12+ months in lower-stress areas.
- Dissolver gets "lost" in surrounding soft filler. When hyaluronidase (Hyaluronidase) is injected into the fold, it diffuses through the path of least resistance — which is the soft, non-encapsulated filler around the lump, not the dense capsule itself. This is why patients describe the same outcome: the fold gets deeper and softer, but the hard cord is still there.
Key Insight: A failed dissolution attempt at the nasolabial fold is rarely a dose problem — it's a delivery problem. Without ultrasound to map where the enzyme is actually going, repeat injections often deepen the fold further while the encapsulated lump remains untouched. This is why FILLER REVISION evaluates every nasolabial fold lump with ultrasound before deciding whether enzymatic dissolution is even the right tool.
When It's Likely Just Normal Texture
The following situations typically require no intervention:
- You're still within 2–4 weeks post-injection and residual swelling hasn't fully resolved
- The texture feels soft and uniform with no distinct lumps
- It compresses easily under finger pressure
- It doesn't affect facial expression or appearance
- It gradually becomes less noticeable over time
Key Insight: Hyaluronic acid fillers, even when perfectly placed, can sometimes be palpable in areas where skin is thin and the underlying structure is linear. Feeling something doesn't automatically mean something is wrong.
When You Should Seek Evaluation
These signals suggest a visit to a specialist is warranted:
- The lump persists unchanged or worsens beyond 4 weeks post-injection
- The lump is visible—you can see a ridge under certain lighting or angles
- The texture is becoming harder over time rather than softer
- There is tenderness or intermittent pain on palpation
- The lump's location doesn't match where the filler was originally injected (suggesting migration)
- Skin color changes appear over the area
The Diagnostic Value of Ultrasound
High-resolution ultrasound provides critical information in the nasolabial fold region:
- Distribution pattern: Is the filler evenly spread or clumped into deposits?
- Encapsulation status: Has a fibrous capsule formed around the filler?
- Depth assessment: Is the filler at the correct tissue plane, or is it too superficial or too deep?
- Inflammatory reaction: Is there tissue inflammation surrounding the filler?
- Volume estimation: How much residual filler remains and where is it distributed?
This diagnostic clarity is essential because different causes require fundamentally different treatment strategies.
Treatment Strategies by Lump Type
For encapsulated lumps: Dissolving enzymes typically cannot penetrate the fibrous capsule. Ultrasound-guided pinhole extraction provides a more reliable solution.
For filler aggregation without encapsulation: If the filler is hyaluronic acid and not encapsulated, precisely targeted enzyme injection under ultrasound guidance may be effective.
For displaced filler: Ultrasound must first confirm the filler's actual location before an extraction strategy can be designed. Blind treatment risks missing the displaced material entirely.
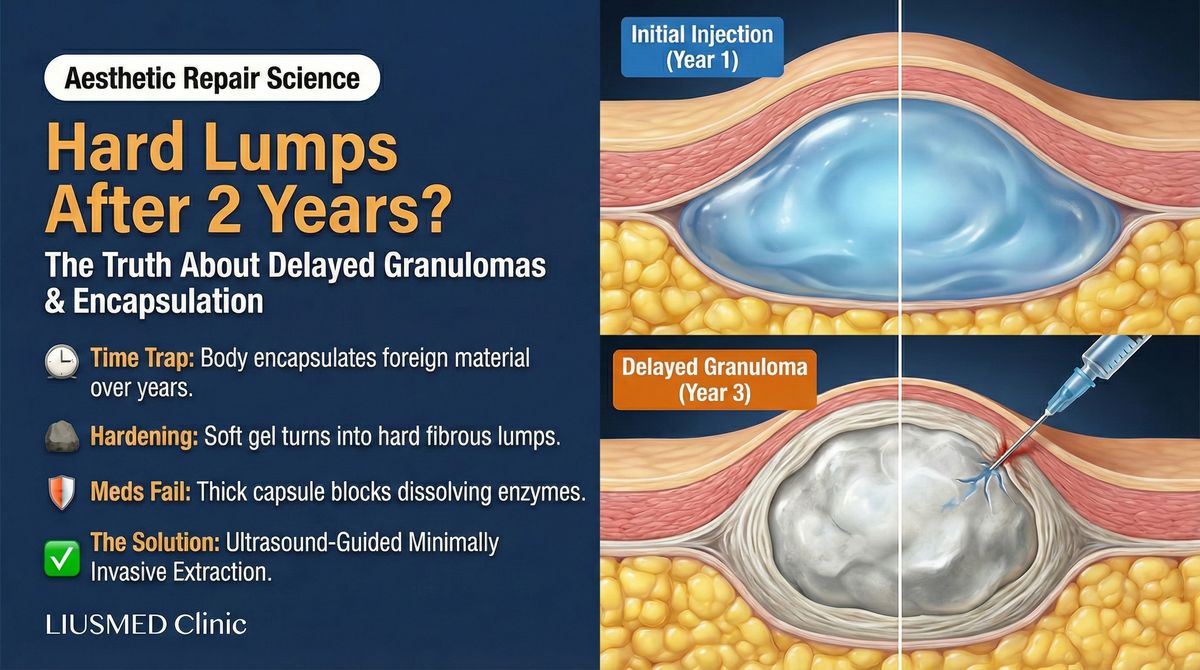
For inflammatory or granulomatous lumps: Inflammation must be controlled first, then a decision is made about whether the filler needs removal. See lumps appearing years after injection for more detail.
When Dissolution Deepens the Fold Instead of Fixing the Lump: The FILLER REVISION Approach
At FILLER REVISION, patients with nasolabial fold lumps frequently describe the same frustrating experience: dissolution reduced the surrounding normal filler while the hard lump remained, making the fold appear deeper and the lump more prominent. This happens because encapsulated filler resists enzymatic breakdown, while the softer surrounding filler dissolves readily. Our approach uses ultrasound to first determine whether the lump is truly encapsulated or simply aggregated, then applies the appropriate treatment: precise enzyme delivery for accessible deposits, or pinhole extraction for encapsulated material. This targeted strategy removes the lump without sacrificing the beneficial volume that fills the fold.
Prevention: Nasolabial Fold Injection Best Practices
- Appropriate product selection: The nasolabial fold requires products with adequate support but not excessive firmness
- Correct depth: Too superficial makes the filler easily palpable; too deep compromises the visible result
- Avoid overfilling: The nasolabial fold has limited tissue space—overfilling increases lump risk significantly
- Even distribution: Injection technique should ensure filler spreads uniformly along the fold rather than accumulating in one spot
If you've already tried treatment for nasolabial fold lumps without success, FILLER REVISION specializes in exactly these cases. Our ultrasound assessment distinguishes normal texture from true complications, and our targeted approach removes lumps without deepening the fold.
Frequently Asked Questions
How do I tell if it's normal filler texture or actually an encapsulated lump?
Three differences usually settle it. (1) Compressibility: normal filler yields under firm finger pressure and rebounds — an encapsulated cord stays rigid no matter how hard you press. (2) Border definition: normal filler texture blends into surrounding tissue; an encapsulated lump has a sharp, clearly defined edge you can trace with a fingertip. (3) Timeline: normal texture becomes softer and less noticeable over weeks to months — encapsulation moves the opposite direction, getting harder and more sharply defined. If you have any combination of "firm + sharp-edged + getting worse over time," it is very likely encapsulated. Ultrasound (Ultrasonography) is the primary way to confirm definitively, but these three features are reliable enough to justify booking an evaluation rather than waiting another six months.
My doctor said "just wait and observe" — should I keep waiting or seek a second opinion?
The "wait and see" approach makes sense for the first 8–12 weeks, but it is the wrong answer past that window if the lump is unchanged or getting harder. Encapsulated filler does not spontaneously resolve — the fibrous capsule continues to mature and the lump becomes progressively harder to treat. Patients who wait 1–2 years on observation alone often arrive with denser, larger lumps that require more extensive extraction than if they had been evaluated at the 3-month mark. A reasonable rule: if the lump is unchanged at 12 weeks post-injection, get an ultrasound evaluation regardless of what your original injector advises. A second opinion does not commit you to treatment — it gives you the imaging-based information needed to decide.
After ultrasound-guided extraction, will my nasolabial fold need to be refilled?
Often not — and that surprises patients who assumed extraction would leave them looking older. Here is why: an encapsulated lump occupies space but does not contribute to the cosmetic correction of the fold. When the lump and its capsule are removed, the surrounding soft tissue typically settles back into a more natural contour. In FILLER REVISION's case experience, most patients are satisfied without immediate refilling. For those who do want additional volume, we recommend waiting at least 3 months after extraction so tissue has fully healed and any residual swelling has resolved. Future filler should be placed under ultrasound guidance, in smaller volumes per pass, and ideally with a product that has a known lower encapsulation profile in the nasolabial region.