When Your Immune System Decides "This Doesn't Belong Here"
If a hard, red, persistently swollen nodule has appeared at your injection site — months or even years after treatment — you may be frightened and confused. Your doctor may have tried steroids, antibiotics, or other medications with only temporary results. Understanding what is actually happening inside your tissue is the first step toward finding a solution that lasts. This is your immune system launching a full-scale war against a foreign material it cannot break down. In medical terminology, this reaction is called a foreign body granuloma, a well-characterized complication that can occur with all injectable dermal fillers (Lemperle et al., 2009).
Many patients panic when they first experience a granuloma: "Is it a tumor?" or "Was there something wrong with the filler?" In reality, a granuloma is a normal immune defense mechanism — but in the context of dermal fillers, this defense becomes an endless war of attrition with no winner.
Key Insight: At FILLER REVISION, our clinical experience confirms that a foreign body granuloma is neither an allergic reaction nor an infection. It is your immune system's chronic siege strategy — an attempt to "digest" a foreign substance it can never break down. Recognizing this distinction is essential because the treatment path for granulomas is fundamentally different from treating infection or allergy.
How the Immune System Recognizes Foreign Materials
The First Line of Innate Immunity
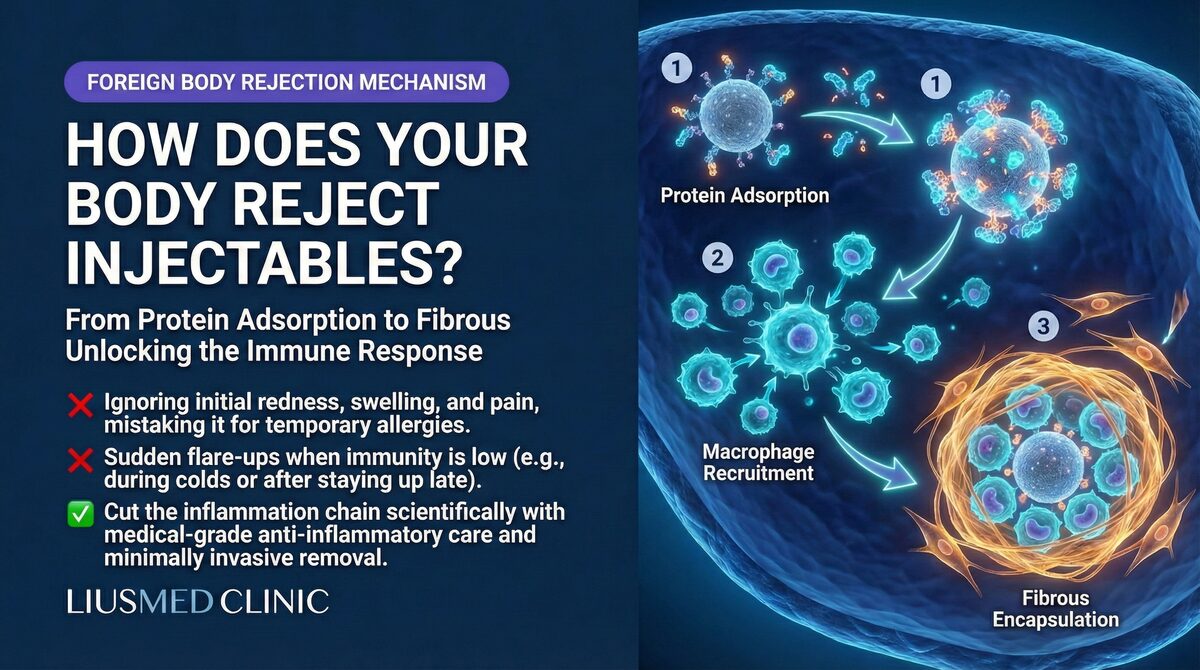
When any foreign substance enters tissue, the immune response follows a precise, stepwise escalation:
-
Damage signal release: The injection itself causes micro-tissue injury. Damaged cells release Danger-Associated Molecular Patterns (DAMPs), alerting nearby immune cells.
-
Neutrophil first responders: Within hours, neutrophils arrive at the injection site and attempt to engulf and destroy the foreign material. Against small invaders like bacteria, this is usually sufficient.
-
Macrophage takeover: When neutrophils cannot handle the material — filler particles are far larger than bacteria — monocytes are recruited from the bloodstream and differentiate into macrophages to take over the cleanup.
-
The "can't digest it" dilemma: Macrophages attempt to phagocytose filler particles, but these synthetic materials cannot be broken down by lysosomal enzymes. The macrophage is stuck — it has captured the enemy but cannot destroy it.
From Acute Inflammation to Chronic Warfare
This "can't digest it" dilemma is the turning point of the entire story.
← Swipe to see more →
| Immune Response Phase | Timeline | Primary Cells | Clinical Presentation |
|---|---|---|---|
| Acute inflammation | Hours to days | Neutrophils | Mild redness, normal post-injection reaction |
| Chronic inflammation onset | Days to weeks | Macrophages | Persistent swelling, pressure sensitivity |
| Giant cell formation | Weeks to months | Multinucleated giant cells | Palpable hard nodule |
| Granuloma maturation | Months to years | Organized granuloma | Firm mass, skin discoloration |
| Fibrotic encapsulation | Years | Fibroblasts | Permanent hard lump, tissue distortion |
The Molecular Mechanisms of Granuloma Formation
Giant Cell Fusion: A Desperate Escalation Strategy
When individual macrophages cannot engulf larger filler particles, the immune system activates an unusual strategy: multiple macrophages fuse into a single, massive multinucleated giant cell, also known as a Foreign Body Giant Cell (FBGC).
This fusion process is regulated by multiple cytokines:
- IL-4 and IL-13: Secreted by T-helper cells, these promote macrophage fusion
- RANKL: Promotes formation of osteoclast-like giant cells
- MCP-1 (CCL2): Continuously recruits more monocytes from the bloodstream
- TNF-alpha: Maintains the chronic inflammatory environment
Key Insight: The foreign body giant cell is the immune system's "ultimate weapon" — when regular troops cannot handle the enemy, soldiers fuse into a giant. But even a giant cannot digest synthetic filler materials.
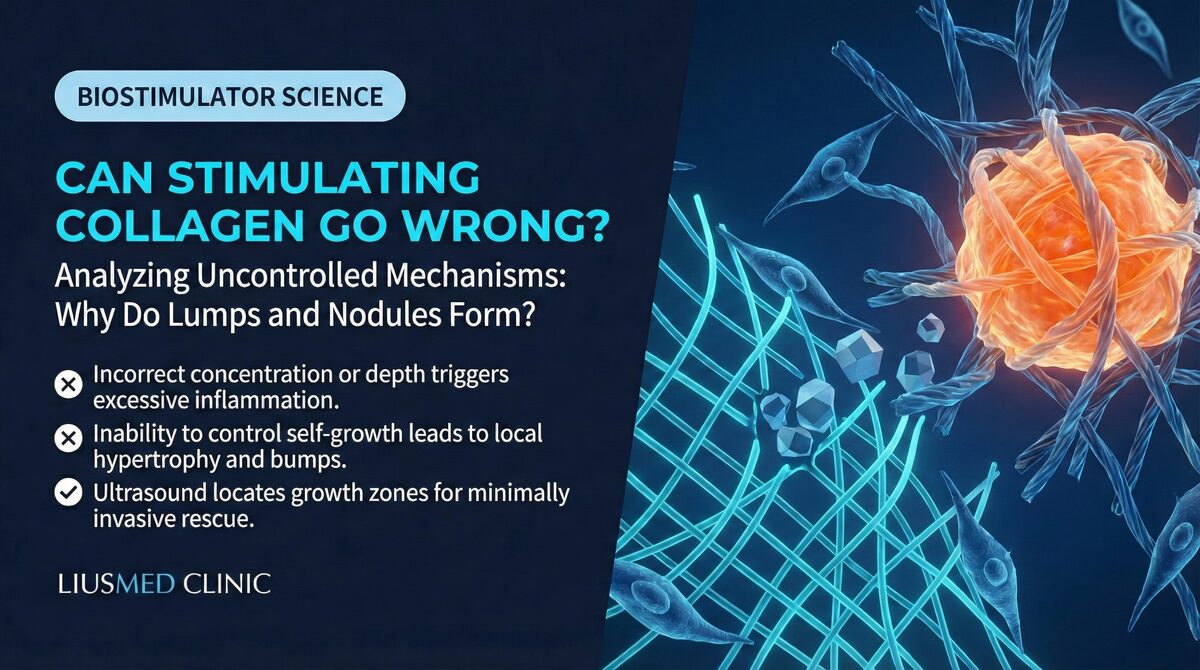
The Organizational Structure of a Granuloma
A mature foreign body granuloma has a highly organized structure, much like a fortress built around an enemy:
- Core zone: Filler particles tightly surrounded by foreign body giant cells and macrophages
- Lymphocyte ring: T-cells and B-cells forming an outer defense perimeter, continuously secreting inflammatory mediators
- Fibroblast layer: The outermost layer, depositing collagen to form a fibrous capsule — effectively building a wall around the enemy
- Neovascularization: New blood vessels supplying the "battlefield" with a continuous stream of immune cells and nutrients
This explains why granulomas feel hard and well-defined to the touch — they are not a chaotic mass of tissue, but a carefully constructed immune fortification.
Granuloma Risk Differences Among Filler Types
Not all fillers trigger granulomas at the same rate. The chemical composition, particle size, and surface properties of each material influence the intensity of the immune response.
← Swipe to see more →
| Filler Type | Granuloma Incidence | Typical Onset | Mechanism |
|---|---|---|---|
| Hyaluronic acid (HA) | 0.01–0.1% | 6–24 months | Often related to cross-linker residues or protein contamination |
| Poly-L-lactic acid (PLLA/Sculptra) | 0.5–5% | 3–18 months | Particulate form readily triggers giant cell response |
| Polycaprolactone (PCL/Ellanse) | 1–3% | 6–24 months | Large microsphere surface area increases immune contact |
| Calcium hydroxylapatite (CaHA/Radiesse) | 0.5–2% | 3–12 months | Uneven microsphere degradation can trigger reaction |
| Silicone / permanent fillers | 5–15% | Months to decades | Permanent foreign body reaction, cannot be metabolized |
| Autologous fat | 0.1–1% | Months to years | Fat necrosis and oil cyst formation triggers response |
Even supposedly "absorbable" fillers carry a non-zero granuloma risk. Cross-linker residues in HA (Hyaluronic Acid), particle aggregation in PLLA (Poly-L-Lactic Acid), and the surface properties of PCL (Polycaprolactone) microspheres can all become targets that the immune system locks onto. Delayed immune-mediated adverse effects have been documented across all filler categories, often presenting months to years after injection (Alijotas-Reig et al., 2013).
Differentiating Granulomas from Other Filler Lumps
When patients feel a hard lump at an injection site, there can be multiple causes. Accurate differential diagnosis is essential for choosing the right treatment approach.
Common Types of Filler Lumps
- Filler material nodules: Visible lumps from filler aggregation or superficial placement, usually without inflammatory signs
- Encapsulation: Fibrous tissue wrapping around filler, forming a smooth, mobile hard lump
- Biofilm-related swelling: Recurrent swelling caused by bacterial biofilm, often with intermittent flare-up patterns
- Foreign body granuloma: Immune-mediated chronic inflammatory nodule, typically firm with poorly defined borders merging into surrounding tissue
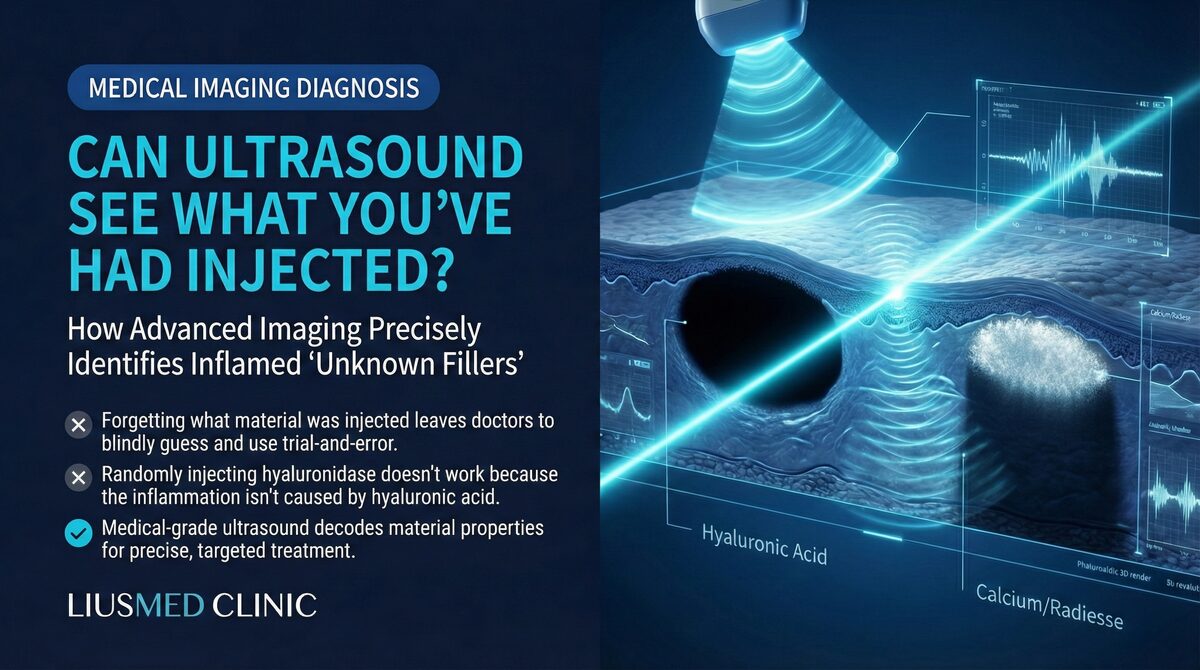
The Diagnostic Value of High-Resolution Ultrasound (Ultrasonography)
Among these different causes, high-resolution ultrasound is the preferred non-invasive diagnostic tool. Ultrasound can reveal:
- The exact location, depth, and distribution of filler material
- The degree of surrounding tissue inflammation and blood flow changes
- Whether capsular structures or liquefactive necrosis are present
- Aggregation patterns of filler particles
This "see before you treat" approach is the key to avoiding blind treatments that cause additional harm. To learn more about ultrasound in filler diagnosis, see the filler repair evaluation process.
Clinical Implications for Revision Patients
For patients who arrive at FILLER REVISION with granulomas, the diagnostic journey is often just as important as the treatment itself. Many have been through multiple rounds of steroids or antibiotics without lasting improvement, and some have been misdiagnosed entirely. At FILLER REVISION, high-resolution ultrasound enables us to differentiate granulomas from other causes of filler lumps — biofilm-related swelling, simple encapsulation, or filler aggregation — each of which requires a different treatment approach. Once a granuloma is confirmed, the treatment logic becomes clear: the foreign body driving the immune response must be removed. Ultrasound-guided extraction targets the filler deposits at the granuloma core, removing the immune target and allowing the inflammatory cycle to resolve.
Why Traditional Medical Treatments Have Limited Effectiveness
The Temporary Nature of Steroid Injections
Local steroid injection (such as Triamcinolone) is the most common first-line treatment for granulomas. Steroids work by suppressing inflammatory responses and immune cell activity to reduce granuloma volume.
The problem is that steroids only temporarily suppress the immune response without removing the root cause — the filler material itself. Once steroid effects wear off, the immune system re-engages, and the granuloma often recurs.
Worse, repeated steroid injections can cause serious side effects:
- Local fat atrophy (skin depression)
- Skin thinning and telangiectasia
- Pigmentation abnormalities
- Impaired tissue repair capacity
The Limitations of 5-FU (5-Fluorouracil)
5-Fluorouracil (5-FU), as an antimetabolite, can inhibit fibroblast proliferation and has some effect on fibrosis-dominant granulomas. However, it also cannot eliminate existing filler material, and in treating collagen stimulator nodules, its results are often disappointing.
The Misuse of Antibiotics
When granulomas are misdiagnosed as infections, patients may receive multiple rounds of antibiotics. Since granulomas are fundamentally immune reactions rather than infections, antibiotics are not only ineffective but can cause side effects such as gut dysbiosis and delay appropriate treatment.
Key Insight: All medical treatments "manage symptoms" rather than "solve the problem." As long as the filler material triggering the immune response remains in the tissue, the granuloma retains the potential to recur. The logic of a cure is simple — remove the foreign body.
Why Physical Removal Is the Definitive Solution: An Immunological Perspective
Immunology teaches us a simple truth: a foreign body granuloma exists because of the foreign body. Remove the foreign body, and you remove the target that the immune system is continuously attacking.
However, removing filler is not as straightforward as it might seem. Traditional methods include:
- Hyaluronidase dissolution: Only effective for HA, and even then, the enzyme often cannot penetrate the capsule to reach the filler core in encapsulated cases (see Encapsulation: Why Dissolvers Fail)
- Blind squeezing or aspiration: Operating without seeing the exact filler location risks damaging normal tissue
- Surgical excision: While effective at removing filler, the resulting scars and tissue damage may be worse than the original problem
Ultrasound-guided minimally invasive extraction offers a more precise option. Under real-time high-resolution ultrasound guidance, the physician can pinpoint every filler deposit's location and depth, extracting material through a tiny pinhole incision while maximizing preservation of surrounding normal tissue.
This "see before you treat" principle not only improves clearance rates but also dramatically reduces collateral tissue damage. Learn more about the filler lump extraction technique.
Prevention and Early Recognition of Granulomas
Strategies to Reduce Granuloma Risk
While granuloma formation cannot be completely prevented, the following measures can reduce risk:
- Choose quality filler products: Products with low impurity levels and stable manufacturing are less likely to trigger immune reactions
- Avoid excessive injection volumes: The more filler material in the tissue, the greater the burden on the immune system
- Strict aseptic technique: Reducing bacterial contamination prevents biofilm formation and subsequent biofilm-related swelling
- Carefully assess injection sites: Areas with pre-existing foreign material carry higher risk with repeat injection
When Should You Seek Medical Attention?
If you experience any of the following after filler injection, seek professional evaluation promptly:
- A gradually enlarging firm nodule at the injection site
- A nodule accompanied by persistent redness or increased skin temperature
- New lumps appearing months to years after injection
- Sudden changes in a previously stable injection area
Early detection and accurate diagnosis can prevent unnecessary medication cycles and allow intervention before tissue damage becomes extensive. If you are considering filler repair, please contact us for an evaluation.
Understanding the Immune Mechanism — FILLER REVISION Can Help
Foreign body granulomas are not medical accidents — they are your immune system activating an ancient defense strategy against a substance it cannot digest. Understanding this mechanism helps you make rational treatment decisions:
- Medication can temporarily control symptoms but cannot eliminate the cause
- Repeated pharmacotherapy may cause additional tissue damage
- Physical removal of the foreign body is the primary way to break the immune response cycle
- Precise image guidance makes the removal process safer and more effective
Your immune system is faithfully doing its job to protect you. The solution is not to suppress it, but to remove the reason it keeps fighting. At FILLER REVISION, Dr. Ta-Ju Liu uses ultrasound-guided extraction to remove the immune target precisely — ending the war your body can never win on its own.
Frequently Asked Questions
Is a foreign body granuloma a tumor, an infection, or an allergic reaction?
No. A foreign body granuloma is none of these. It is your immune system's chronic attempt to wall off and "digest" a filler material it cannot break down. Recognizing this distinction matters, because the treatment path for a granuloma is fundamentally different from treating an infection or an allergy.
Why do my granuloma lumps keep coming back after steroid injections?
Steroids only temporarily suppress the inflammation and immune cell activity to shrink the lump. They do not remove the root cause — the filler material itself. Once the steroid effect wears off, the immune system re-engages, and the granuloma often recurs. As long as the filler triggering the response stays in the tissue, the granuloma retains the potential to come back.
Which fillers are most likely to cause a granuloma, and which are least likely?
All filler types carry some granuloma risk, but the rates differ. Permanent fillers such as silicone have the highest reported incidence (5–15%), while hyaluronic acid has the lowest (0.01–0.1%). Even "absorbable" fillers are not zero-risk: cross-linker residues in HA, particle aggregation in PLLA (Sculptra), and the surface properties of PCL (Ellanse) microspheres can all become immune targets.
How can my doctor tell whether my lump is actually a granuloma and not something else?
A hard lump at an injection site can have several causes — filler aggregation, fibrous encapsulation, biofilm-related swelling, or a true granuloma — and each needs a different treatment. High-resolution ultrasound is the preferred non-invasive tool to tell them apart: it shows the exact location, depth and distribution of the filler, the degree of surrounding inflammation, and whether capsular structures are present. This "see before you treat" approach helps avoid blind treatments that cause additional harm.
If medications don't cure a granuloma, what is the definitive solution?
Because a granuloma exists only because of the foreign body, removing that filler removes the target the immune system keeps attacking. The primary definitive treatment is physical removal of the filler driving the response. Ultrasound-guided minimally invasive extraction lets the physician pinpoint each deposit's location and depth and remove material through a tiny pinhole incision, while preserving surrounding normal tissue as much as possible.
When should I see a doctor about a lump after filler?
Seek professional evaluation promptly if you notice a gradually enlarging firm nodule at the injection site, a nodule with persistent redness or increased skin temperature, new lumps appearing months to years after injection, or sudden changes in a previously stable area. Early detection and accurate diagnosis can prevent unnecessary medication cycles and allow intervention before tissue damage becomes extensive.