Why Does My Filler Keep Swelling Months or Years After Injection?
If you are here, you are probably trapped in a frustrating cycle: your filler area swells up, your doctor prescribes antibiotics, the swelling goes down — and then it comes back again. You may have gone through this loop three, four, or more times and are starting to wonder whether anyone truly understands what is happening inside your face.
This frustrating cycle of recurring swelling is one of the most misunderstood complications in aesthetic medicine. In most cases, the cause is not a new infection—it is a biofilm that has been living silently on the surface of your filler since the day it was injected.
What Is a Biofilm?
The Invisible Colony
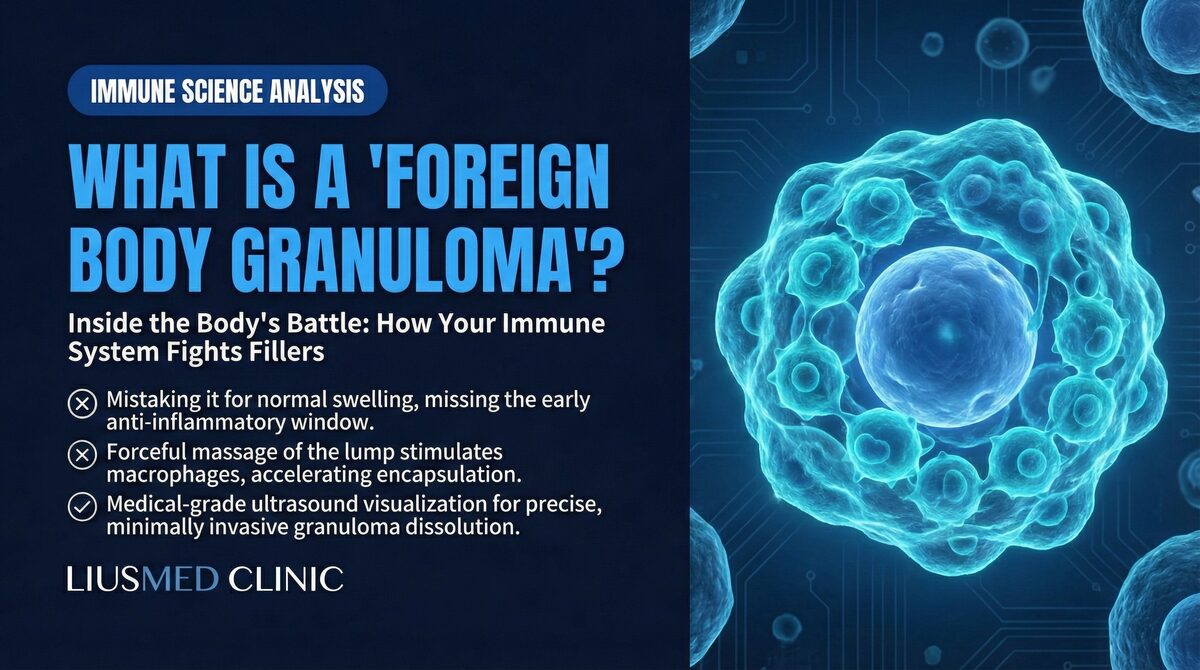
A biofilm is a structured community of bacteria that attaches to a surface and encases itself in a self-produced protective matrix. This matrix—composed of polysaccharides, proteins, and extracellular DNA—functions as a shield that protects the bacterial colony from the immune system, antibiotics, and environmental threats.
Think of a biofilm like a coral reef in miniature. Individual bacteria are like the coral polyps—small and vulnerable on their own. But once they organize into a colony and secrete their protective matrix, they become a resilient, self-sustaining structure that is extraordinarily difficult to eradicate.
Key insight: At FILLER REVISION, our clinical experience confirms that a biofilm is not a conventional infection. It is an organized, protected colony of bacteria living in a dormant state on a foreign surface — in this case, your filler. Recognizing this distinction is the critical first step toward a treatment that actually works.
How Does Biofilm Form on Filler?
Biofilm formation on dermal fillers follows a predictable sequence:
-
Contamination at injection: Bacteria from the skin surface, the injection needle, or the clinical environment are introduced into the tissue along with the filler material. Even with strict aseptic technique, complete sterility is impossible.
-
Attachment: Within hours, bacteria attach to the filler surface. All filler materials—hyaluronic acid, polycaprolactone, poly-L-lactic acid, calcium hydroxylapatite—provide surfaces to which bacteria can adhere.
-
Colony formation: Attached bacteria begin to multiply and communicate through chemical signaling (quorum sensing). They coordinate their behavior and begin secreting the protective extracellular matrix.
-
Maturation: Over days to weeks, the biofilm matures into a complex three-dimensional structure with channels for nutrient and waste exchange. The colony establishes a stable, self-sustaining ecosystem.
-
Dormancy: Once mature, the majority of bacteria within the biofilm enter a metabolically dormant state. They are alive but not actively dividing or producing the metabolic byproducts that would trigger an immune response.
Why Do Antibiotics Fail Against Biofilm?
The Dormancy Problem
Conventional antibiotics work by disrupting essential bacterial processes—cell wall synthesis, protein production, DNA replication. These mechanisms all require the bacteria to be actively growing and dividing. Dormant bacteria within a biofilm are metabolically inactive, making them essentially invisible to antibiotics.
This is analogous to trying to stop a factory by cutting its power supply. If the factory is running, cutting power will shut everything down. But if the factory is already closed for the night, cutting power has no effect—the machinery is already idle.
Key insight: Antibiotics can kill the active bacteria that escape from the biofilm surface, which is why they temporarily reduce swelling. But they cannot penetrate the biofilm matrix or kill the dormant core population. This is why the symptoms always return.
The Protective Matrix
Even if some bacteria within the biofilm are metabolically active, the extracellular matrix acts as a physical and chemical barrier to antibiotic penetration. Studies have shown that bacteria within biofilms can be 100 to 1,000 times more resistant to antibiotics than the same bacteria in a free-floating (planktonic) state.
The matrix achieves this protection through multiple mechanisms:
- Physical barrier: The dense polysaccharide matrix physically blocks large antibiotic molecules from reaching the bacteria
- Enzymatic degradation: Some biofilms contain enzymes that break down antibiotics before they can reach their targets
- Chemical microenvironment: The interior of a biofilm has altered pH, oxygen levels, and nutrient concentrations that reduce antibiotic effectiveness
- Efflux pumps: Bacteria within biofilms upregulate molecular pumps that actively expel antibiotics from their cells
What Triggers Biofilm Flare-Ups?
The Immune Balance Theory
If the biofilm is dormant, why does swelling occur at all? The answer lies in the dynamic balance between the biofilm and the host immune system.
Under normal conditions, the immune system maintains a low-level surveillance of the biofilm. The protective matrix prevents the immune system from eliminating the colony, but the immune system keeps the biofilm in check, preventing it from expanding aggressively. This creates an uneasy equilibrium—the biofilm survives but does not cause symptoms.
This balance can be disrupted by events that alter the immune system's capacity:
- Systemic illness: Influenza, COVID-19, or other infections temporarily redirect immune resources, allowing the biofilm to reactivate
- Dental procedures: Dental work can introduce transient bacteremia (bacteria in the bloodstream) that seeds additional bacteria to the biofilm site
- Vaccination: The immune response triggered by vaccination can cause cross-reactive inflammation at the biofilm site
- Hormonal changes: Menstrual cycle fluctuations, pregnancy, or hormonal medications can modulate immune function
- Physical trauma: Facial massage, aggressive skincare treatments, or dental work near the filler site can physically disturb the biofilm
- Stress and fatigue: Chronic stress suppresses immune function, potentially allowing biofilm reactivation
Key insight: Biofilm flare-ups are not new infections. They represent a temporary shift in the balance between the dormant bacterial colony and the immune system. This is why they resolve temporarily with antibiotics but inevitably recur.
How Is Biofilm Diagnosed?
Clinical Suspicion
Biofilm should be suspected whenever a patient presents with:
- Recurring swelling in a previously injected area
- Swelling that responds to antibiotics but returns after completing the course
- Late-onset inflammation (months to years after injection)
- Low-grade tenderness or firmness at the filler site without classic signs of acute infection (no fever, no purulent discharge)
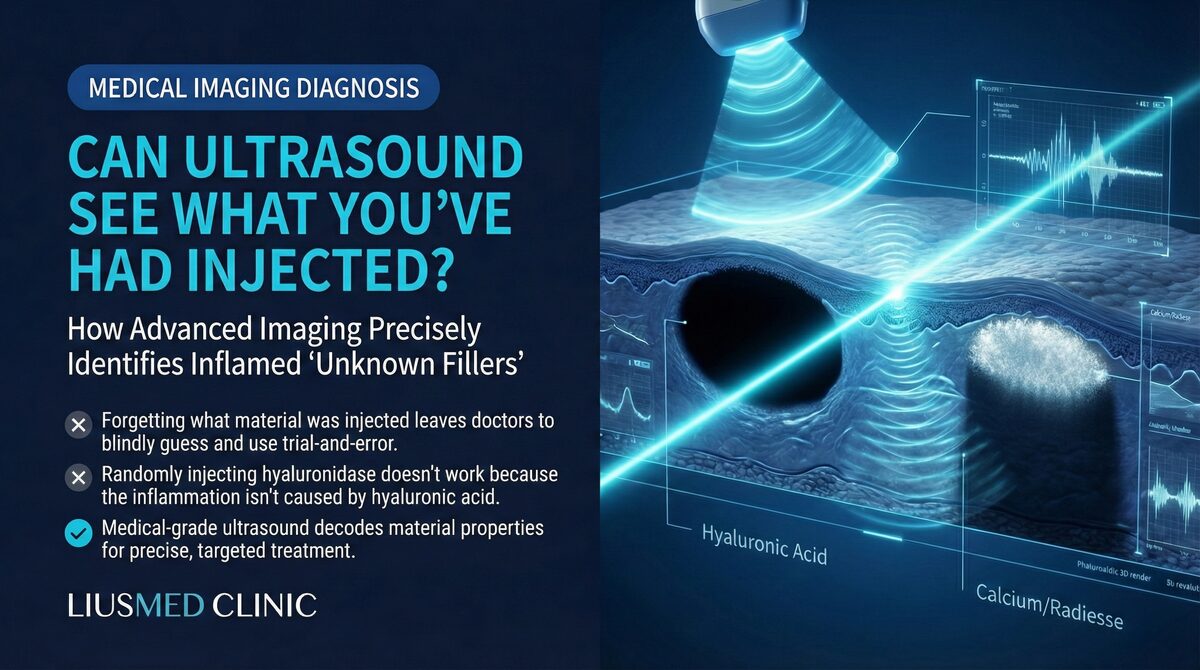
Imaging Confirmation
High-frequency ultrasound can reveal characteristic findings associated with biofilm-contaminated filler:
- Irregular fluid collections surrounding the filler material
- Altered echogenicity of the filler compared to uncontaminated material
- Surrounding soft tissue edema and inflammatory changes
- Subtle capsule thickening around the filler deposit
It is important to note that biofilm itself is not directly visible on ultrasound. The diagnosis is made based on the clinical pattern (recurring inflammation associated with filler) combined with imaging findings that are consistent with chronic low-grade infection.
Clinical Implications for Revision Patients
For patients caught in the recurring swelling cycle, understanding biofilm science changes everything about the treatment approach. At FILLER REVISION, we see patients who have endured months or years of repeated antibiotic courses without lasting relief. The reason is now clear: antibiotics manage the symptoms of biofilm flare-ups but cannot reach the dormant colony protected within its matrix. This is why our approach focuses on identifying and physically removing the contaminated filler — the surface on which the biofilm lives. Once the colonized material is extracted under ultrasound guidance, the cycle breaks permanently. The immune system clears the remaining exposed bacteria without difficulty, and the pattern of recurring swelling stops.
Why Physical Removal Is the Primary Definitive Treatment
The Logic of Removal
Since the biofilm lives on the surface of the filler material, the primary way to definitively eliminate the biofilm is to remove the surface on which it resides. This means physically extracting the contaminated filler.
Consider the analogy of mold growing on a wall. You can spray the wall with antifungal chemicals repeatedly, and the visible mold may disappear temporarily. But as long as the contaminated wall material remains, the mold will always grow back. The definitive solution is to remove the affected wall section entirely.
Key insight: Removing the filler removes the biofilm's home. Without a surface to colonize, the remaining bacteria are exposed to the immune system and antibiotics and are rapidly eliminated.
The Extraction Process
Ultrasound (Ultrasonography)-guided filler extraction allows the physician to:
- Visualize the exact location and extent of contaminated filler material
- Access the filler deposit through a minimally invasive approach
- Extract the material along with its biofilm-colonized surface
- Verify completeness of removal through real-time ultrasound imaging
- Confirm resolution of inflammatory changes on follow-up imaging
For hyaluronic acid fillers, hyaluronidase may be used as an adjunct to soften the material before extraction. However, for non-HA (Hyaluronic Acid) fillers (Ellanse, Sculptra, Radiesse), physical extraction is the primary option, as no chemical dissolver exists.
What Happens After Biofilm Removal?
Once the contaminated filler is removed, the cycle of recurring swelling stops. The immune system clears the remaining planktonic bacteria without difficulty. Most patients experience:
- Immediate reduction in swelling and tenderness within days
- Complete resolution of inflammatory symptoms within two to four weeks
- No recurrence of the characteristic swelling pattern
A short course of antibiotics may be prescribed after extraction to address any bacteria released during the removal process. Unlike the endless cycles of antibiotics for intact biofilm, this single post-extraction course is typically curative.
Can Biofilm Be Prevented?
Complete prevention is not currently possible, as some degree of bacterial contamination is inherent to any injection procedure. However, risk can be minimized through:
- Strict aseptic technique during injection
- Skin preparation with appropriate antiseptic solutions
- Avoidance of injection through areas of active skin infection or inflammation
- Single-use needles and cannulas for each injection site
- Minimizing tissue trauma during the injection process
Frequently Asked Questions
Why don't antibiotics work on biofilm even when my doctor prescribed strong ones?
The issue is not antibiotic potency — it is bacterial state and physical access. Antibiotics work by disrupting active bacterial processes such as cell wall synthesis, protein production, and DNA replication. Inside a mature biofilm, the majority of bacteria are in a metabolically dormant state and are essentially invisible to those drugs. On top of that, the extracellular matrix surrounding the colony acts as both a physical and chemical barrier — studies show biofilm bacteria can be 100 to 1,000 times more resistant to antibiotics than free-floating (planktonic) bacteria. What antibiotics do kill is the small population of active bacteria that escape from the biofilm edge, which is why your swelling temporarily improves. But the dormant core colony remains intact, so the cycle restarts every time immune balance shifts. Switching to a "stronger" antibiotic without removing the contaminated filler usually produces the same pattern — temporary improvement, then recurrence.
How do I tell if my late-onset swelling is biofilm or a new infection?
Three patterns separate biofilm flare-ups from new acute infections. (1) Timeline: new infections appear within days of an event (procedure, trauma); biofilm flare-ups arise months to years after the original injection, often without a clear trigger. (2) Severity: acute infection produces fever, marked redness, warmth, and sometimes purulent discharge; biofilm flare-ups are usually low-grade — diffuse swelling, mild tenderness, no fever. (3) Antibiotic response: new infections typically resolve on a single antibiotic course and stay resolved; biofilm responds temporarily and then recurs in the same anatomic location, often repeating three, four, or more cycles. If you can answer "yes" to any of "swelling 6+ months after injection," "antibiotic-then-recurrence pattern," or "always swells in the same spot," biofilm is the more likely explanation than re-infection. High-frequency ultrasound (Ultrasonography) can confirm by showing irregular fluid collections, altered echogenicity, and capsule thickening around the filler deposit.
Can hyaluronidase dissolve a biofilm-contaminated HA (Hyaluronic Acid) filler?
Partially, and not reliably. Hyaluronidase only breaks down the HA gel itself — it has no effect on the biofilm matrix or the dormant bacteria living on its surface. When the gel dissolves, the released biofilm fragments can disperse into surrounding tissue and may even trigger a new inflammatory flare-up before the symptoms eventually settle. For non-HA fillers (Ellanse / Polycaprolactone, Sculptra / Poly-L-lactic acid, Radiesse / Calcium hydroxylapatite), no chemical dissolver exists, so dissolution is not even an option. At FILLER REVISION we treat biofilm-suspected cases by ultrasound-guided physical extraction of the contaminated material — with hyaluronidase used only as an adjunct to soften HA gel just before removal, not as standalone therapy. Removing the colonized surface is what actually ends the cycle; chemical dissolution alone tends to convert a slow recurring problem into a faster, more diffuse one.
Break the Cycle with FILLER REVISION
If you are experiencing recurring swelling in a previously injected area, you may be dealing with a biofilm that antibiotics alone cannot resolve. At FILLER REVISION, Dr. Ta-Ju Liu uses ultrasound-guided imaging to identify contaminated filler deposits and extract them precisely — removing the biofilm's home and ending the cycle for good.