
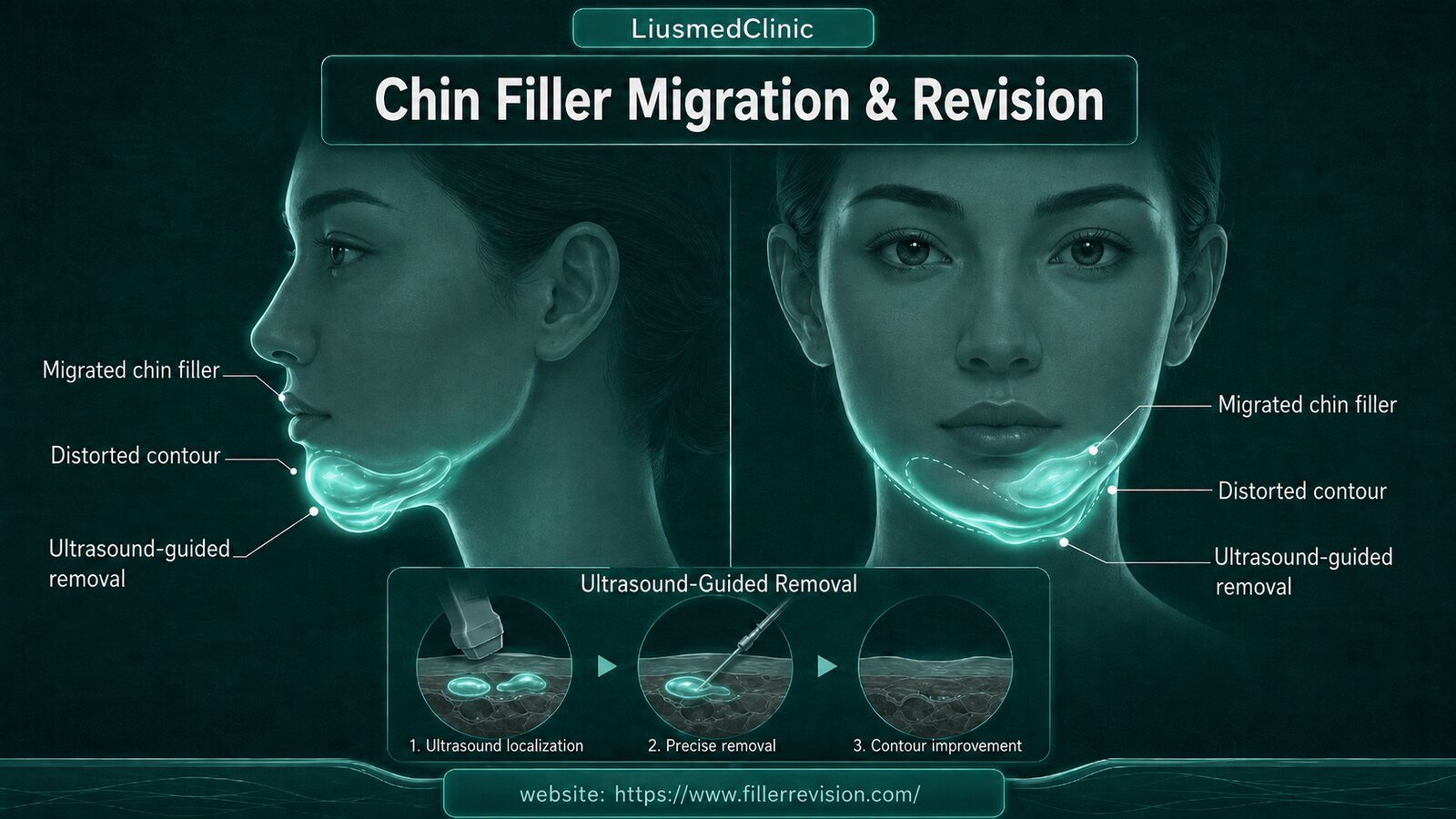
Chin Filler Migration, Contour Distortion & Lump Repair
'I had HA put in my chin — so why is it slowly getting longer, crooked, and drifting down below the chin?' 'My chin feels stiff and foreign, like a hard cord.' That's how many people arrive. The problem with chin filler is usually not the amount, it's position and migration. The chin's skin moves, and the mentalis muscle contracts frequently, so filler is easily pushed downward and sideways, and over time the chin grows longer, crooked, and distorted in contour; too much volume also makes the lower face look bulky and the marionette lines deeper. HA drawing water and spreading, and biostimulators clumping, leave palpable lumps and a foreign-body sensation. The tip of the chin also has the mental artery running through it — a vascular zone to be careful with. I don't rush to add more to reshape it — first I use high-frequency ultrasound to see clearly: which layer the filler has gone to, how far it has migrated, whether it has clumped, and how close it is to the vessels — then decide whether to dissolve, remove, or rebuild the contour's support.
Common Symptoms
Why chin filler tends to migrate, distort, and clump
The chin is a very mobile area — speaking, chewing, and expression all rely on frequent contraction of the mentalis, and that constant muscular push squeezes filler downward and sideways, over time causing migration, a longer and crooked chin, and a distorted contour. When it's overfilled, the weight and volume make the lower face look bulky and the marionette lines deeper. HA draws water and spreads, slowly diffusing outward; biostimulators (PCL, PDLLA, CaHA) and permanent fillers get encapsulated into hard lumps and remain for many years, with no dissolving enzyme. The tip of the chin has the mental artery running through it, so if the position and depth aren't well controlled, it's a matter of vascular safety as well as migration. The problem is usually not 'not enough' — it's position and migration, which is exactly why you have to see where the material has actually gone first.
Why Traditional Treatments Fail
Why 'add more to reshape' and 'keep injecting hyaluronidase' often aren't enough
When the chin distorts or goes crooked, the common move is to add a bit more to reshape it — but if the root cause is migration or too much volume, more filler only makes the chin heavier, more likely to keep drifting down, and the distortion more obvious. Hyaluronidase: it only works on HA, and lumps sealed in a thick capsule often won't dissolve cleanly; worse, the enzyme tends to dissolve the surrounding normal filler first, leaving the contour more uneven and asymmetric. Biostimulators and permanent fillers have no enzyme at all. Massage can't open a mature capsule, nor pull back material that has already migrated. The problem is usually not 'not enough' — it's not having looked first at which layer the filler went to, how far it migrated, and which kind of lump it is.
“The most common misunderstanding about the chin is that once it goes crooked or grows longer, you add more to reshape it. But the chin's muscles are very mobile, and filler is usually being pushed downward and sideways — add more and it just keeps drifting, only heavier. What usually turns the lightbulb on is seeing on the ultrasound where the material has gone. Seeing where it went and where it's caught first, then deciding to dissolve, remove, or rebuild the contour with support, is far more honest than endlessly adding more.”
Dr. LiuStructure > volume: chin distortion is often migration — see it first, then decide to dissolve, remove, or rebuild
Ultrasound-Guided Pinhole Micro-Extraction
The chin isn't fill-it-when-crooked, reshape-it-when-distorted. The muscles here are very mobile and filler is easily pushed into migration — so we build trust on imaging: ultrasound first shows which layer the material went to, how far it migrated, and how close it is to the vessels, then we decide whether to dissolve, remove, or rebuild the contour with a structural thread lift. We're not trying to make the chin bigger — we're pulling the migration and distortion back, so the contour is clean, symmetric, and natural.
Distortion is often migration, not 'not enough'
The chin's mentalis contracts frequently and pushes filler downward and sideways. Ultrasound first confirms which layer it migrated to and how much, so we deal with what has drifted rather than adding more to cover the distortion.
Tell the lump type first, then dissolve or remove
HA that isn't yet encapsulated can be dissolved precisely under ultrasound guidance; material sealed in a thick capsule, and biostimulators and permanent fillers with no enzyme, are removed precisely through a single-pinhole micro-approach under image guidance.
Rebuild the contour with support, not more drifting filler
After the migrated and excess portions are dealt with, the chin's contour and support are rebuilt with a non-migrating structural thread lift and finished smooth after clean removal — rather than injecting more filler that the muscle just pushes around.
Ultrasound-guided: see where it went first, then decide to dissolve, remove, or rebuild the contour
We treat the migration and the volume themselves. Before anything, high-frequency ultrasound shows clearly: which layer the filler is in, where it has migrated, whether it's encapsulated into a hard lump, and how close it is to the mental artery at the tip of the chin. Once it's clear, we triage: HA that isn't yet encapsulated is dissolved precisely under ultrasound guidance; material sealed in a thick capsule, along with biostimulators and permanent fillers that can't be dissolved, is removed precisely through a single pinhole under image guidance (clinically most of it, roughly 80–90%, depending on fibrosis); after the migrated and excess portions are dealt with, the chin's contour and support are rebuilt with a non-migrating structural thread lift, rather than injecting more filler that the muscle just pushes around. The goal is to pull the migration and distortion back, and bring the chin's contour back to clean, symmetric, and natural.
High-frequency ultrasound to read migration, layers, and the mental artery
Comfort-focused local anesthesia
Dissolve what can be reached, single-pinhole removal for the rest
Structural thread lift to rebuild the contour, finished smooth
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
Not necessarily a matter of the wrong amount — more often it's migration. The chin's mentalis is very mobile, and constant muscular contraction pushes filler downward and sideways, over time making it longer, crooked, and distorted in contour. Ultrasound first shows which layer the material went to and how far it migrated, so we can decide whether to dissolve, remove, or rebuild support — rather than adding more to cover the distortion.
Filler that has already migrated, or even been encapsulated, usually can't be pushed back into place with massage, and forcing it may make things messier. The more direct route is to locate where it went with ultrasound first, then precisely dissolve or remove the migrated and excess portions, rebuilding the contour with a structural thread lift when needed — rather than relying on massage or more filler to correct it.
In the early period after injection, a soft, compressible texture is usually normal; but persistent tightness, a stiff foreign-body sensation, or a palpable lump that won't move usually means it needs treatment. Ultrasound can objectively tell whether it's normal filler, an encapsulated lump, migration, or a granuloma, so we can decide what to do.
It depends on the material and whether it's encapsulated. Only HA has a matching enzyme, and when it's sealed in a thick capsule it often won't dissolve cleanly; the enzyme also tends to dissolve the surrounding normal filler first, leaving the contour more uneven. Biostimulators (PCL, PDLLA, CaHA) and permanent fillers have no dissolving enzyme, so for those stubborn lumps ultrasound-guided physical removal is the more direct route.
That's exactly why we see it clearly and remove precisely. Dealing with the migrated and excess portions usually makes the contour cleaner instead; if the original support was insufficient, we rebuild the chin's three-dimensional contour with a structural thread lift, so it finishes smooth and symmetric after removal rather than collapsing or hollowing.
Our aim is to remove cleanly and evenly, but clinically it's usually around 80–90%, depending on how much fibrosis there is — we don't claim 100%. The point is to see where it went first and remove precisely, leaving the contour and symmetry smooth, rather than repeated attempts that make things messier.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Frankeny A. Dissolving vs. removing fillers in the nose prior to rhinoplasty. American Society of Plastic Surgeons (ASPS) — interview with Richard Reish, MD, FACS (notes that large volumes of the enzyme can cause damage to the surrounding tissues).
- Ianhez M, de Goés E Silva Freire G, Sigrist RMS, et al. Complications of collagen biostimulators in Brazil: Description of products, treatments, and evolution of 55 cases. J Cosmet Dermatol. 2024. (Lumps in 89.1% of 55 cases, complete resolution in only 9.1%, delayed onset in 60%.)
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.