Your "Short-Acting" HA (Hyaluronic Acid) May Last Longer Than You Think
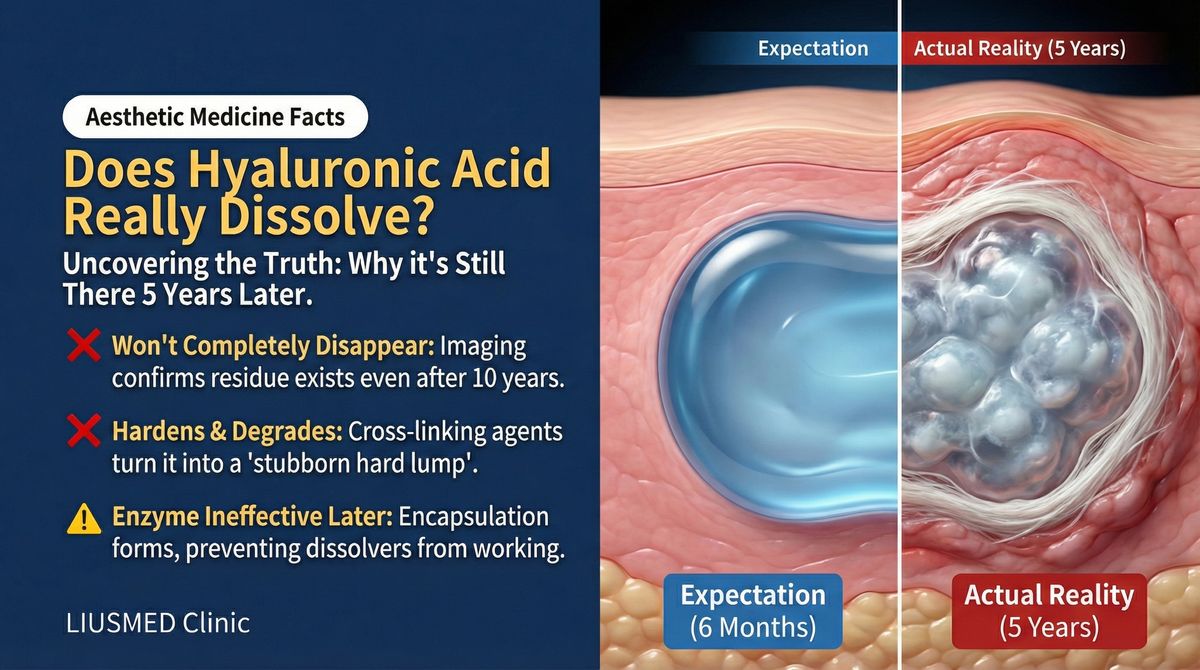
You were reassured that your HA filler was "absorbable" and would be metabolized within 6 to 18 months. Perhaps you are now past that timeline and still feeling or seeing the material. Perhaps hyaluronidase did not fully dissolve it. If you are trying to understand why your "temporary" filler behaves as though it is permanent, the answer lies in the chemistry that made it work in the first place: cross-linking technology. The very modification that gives HA filler its longevity also makes it resist the body's natural degradation — and sometimes resist dissolvers too.
Key Insight: At FILLER REVISION, our clinical experience confirms that native hyaluronic acid has a half-life of only 1–2 days in the body. The reason filler-grade cross-linked HA can persist for 6–18 months or longer is precisely because chemical cross-linking makes it resist enzymatic degradation — but this also means its "absorbability" is dramatically reduced, and residues may persist for years. This is not a rare exception; it is a predictable consequence of the chemistry.
The Chemistry of Cross-Linking
From Native HA to Filler
Native hyaluronic acid is a linear polysaccharide composed of alternating glucuronic acid and N-acetylglucosamine units. Human skin naturally contains abundant HA, but it is continuously degraded by endogenous hyaluronidase, with a half-life of approximately 24–48 hours.
If unmodified HA were injected directly into skin, it would be degraded within days — providing zero filling effect. To create a filler, HA must undergo cross-linking.
BDDE (1,4-Butanediol Diglycidyl Ether): The Most Common Cross-Linker
The vast majority of HA fillers use 1,4-butanediol diglycidyl ether (BDDE) as the cross-linking agent. BDDE's dual epoxide groups can react simultaneously with hydroxyl groups on two HA molecular chains, creating chemical bridges between chains.
← Swipe to see more →
| Cross-Linking Property | Low Cross-Linked Product | High Cross-Linked Product |
|---|---|---|
| BDDE concentration | Lower | Higher |
| Gel firmness (G' value) | Low (soft) | High (firm) |
| Enzymatic resistance | Lower | Higher |
| Labeled duration | 6–9 months | 12–24 months |
| Actual persistence | Possibly 1–3 years | Possibly 2–5+ years |
| Typical use | Lips, tear troughs | Nose bridge, chin, cheekbones |
The Relationship Between Cross-Link Density and Persistence
Higher cross-link density means more chemical bonds between HA chains, creating a tighter three-dimensional network. Research has demonstrated that gel properties and persistence vary significantly among HA fillers depending on cross-linking degree (Edsman et al., 2012). This structure creates a physical barrier against hyaluronidase — enzyme molecules have difficulty accessing HA chains protected within the network interior.
Think of the difference between a sponge and a piece of rubber. A sponge (low cross-linking) has many open pores that water (enzyme) can easily penetrate; rubber (high cross-linking) has a dense structure that water cannot easily infiltrate.
Why Hyaluronidase Cannot Always Fully Dissolve Cross-Linked HA
This is a critical issue that many patients and physicians overlook. Hyaluronidase is considered the "antidote" for HA fillers — inject it and the problem dissolves away. The reality is far more complex.
Factors Affecting Enzymatic Efficiency
Cross-link density: Highly cross-linked products have significantly greater resistance to enzymatic degradation. Clinically, some highly cross-linked HA may require multiple high-dose hyaluronidase injections for only partial dissolution.
Encapsulation effect: Over time, the body forms a fibrous capsule around filler deposits. This capsule becomes a physical barrier preventing enzyme molecules from reaching the filler. For more detail on why encapsulation causes dissolvers to fail.
Filler bolus size: For large filler deposits, enzyme can only degrade from the surface inward. The core region, being farther from the enzyme source, degrades at a significantly reduced rate.
Tissue vascularity: Enzyme activity and diffusion are affected by local blood flow. In areas with sparse vasculature, enzyme delivery efficiency is lower.
Key Insight: Hyaluronidase is not a "magic eraser." For highly cross-linked, encapsulated, or large-bolus HA residues, enzymatic dissolution may be only partially effective, or even completely ineffective. This is why some patients can still feel residual material after multiple hyaluronidase injections.
Clinical Imaging Evidence: The Scale of Persistence
MRI (Magnetic Resonance Imaging) and Ultrasound (Ultrasonography) Findings
Multiple studies using MRI and high-resolution ultrasound to track "expired" HA have found surprising persistence rates:
- Detectable HA residue at 2–3 times the labeled duration
- Residue morphology typically presents as irregular fragments or encapsulated nodules
- In some cases, HA signal is detectable more than 5 years after injection
These findings directly contrast with the myth of complete HA absorption.
Cross-Linking Differences Among HA Brands
Different HA filler brands use different cross-linking technologies and formulations, resulting in significantly different persistence characteristics. Studies on HA filler cohesivity have shown that these rheological differences directly influence clinical behavior and longevity (Sundaram et al., 2015):
← Swipe to see more →
| Technology Platform | Cross-Linking Method | Characteristics | Persistence Tendency |
|---|---|---|---|
| NASHA (Non-Animal Stabilized Hyaluronic Acid) technology | Minimal modification, large particles | Gel particle type | May form palpable boluses |
| Vycross technology | High/low molecular weight mixed cross-linking | High cohesivity, soft | Residue may be more dispersed |
| CPM technology | Continuous optimal cross-linking | Uniform gel | More uniform persistence |
| OBT (Optimal Balance Technology) technology | Optimized balance | High G' value | Structural persistence prominent |
| RHA (Resilient Hyaluronic Acid) technology | Preserved natural structure | High elasticity | Different behavior in dynamic areas |
What Cross-Linking Science Means for Revision Patients
For patients seeking revision at FILLER REVISION, understanding cross-linking chemistry has immediate practical value. The degree of cross-linking in your specific filler product determines how it will respond to hyaluronidase, how likely it is to have formed residual deposits, and whether physical extraction may be necessary. Patients who received highly cross-linked products for structural areas — nose bridge, chin, cheekbones — are statistically more likely to have persistent residues than those who received softer formulations. This is why our assessment begins with ultrasound imaging to confirm what remains, followed by a strategy that accounts for the specific cross-linking characteristics of the material present. A one-size-fits-all approach to HA revision ignores the very chemistry that makes each product behave differently.
Cross-Linking Byproducts and Persistence
Residual Cross-Linker
BDDE is not completely consumed in the cross-linking reaction. Residual unreacted BDDE content is an important indicator of product quality. Regulatory agencies in various countries set upper limits for residual BDDE, but even within standards, trace amounts remain.
Potential effects of residual BDDE:
- May become an antigen recognized by the immune system
- Long-term low-dose tissue exposure effects are not fully established
- May participate in triggering local inflammatory responses
Degradation Intermediates
Cross-linked HA degradation is not a single-step process. During enzymatic and hydrolytic degradation, various intermediates are produced — including HA fragments that still carry cross-linked structures. These fragments are harder to clear than native HA and may persist in tissue long-term.
Implications for Clinical Repair
Understanding the persistence science of cross-linked HA has important implications for repair strategies:
The Necessity of Ultrasound Assessment
Before considering any repair or re-injection, high-resolution ultrasound can:
- Confirm whether old HA residues exist
- Assess residue distribution, size, and degree of encapsulation
- Determine whether residues are causing current symptoms
- Provide precise localization data for subsequent treatment
Learn more about the filler repair evaluation process.
Physical Removal vs. Enzymatic Dissolution
For encapsulated or highly cross-linked HA residues:
- Enzymatic dissolution may have limited effect, requiring repeated high-dose injections
- Excessive hyaluronidase risks dissolving native HA in surrounding normal tissue
- Ultrasound-guided minimally invasive extraction can physically remove residues directly, avoiding the uncertainty of enzymatic dissolution
The Cumulative Risk of Filler Migration (Filler Migration)
Residual cross-linked HA does not just "sit quietly." It may:
- Slowly migrate over time
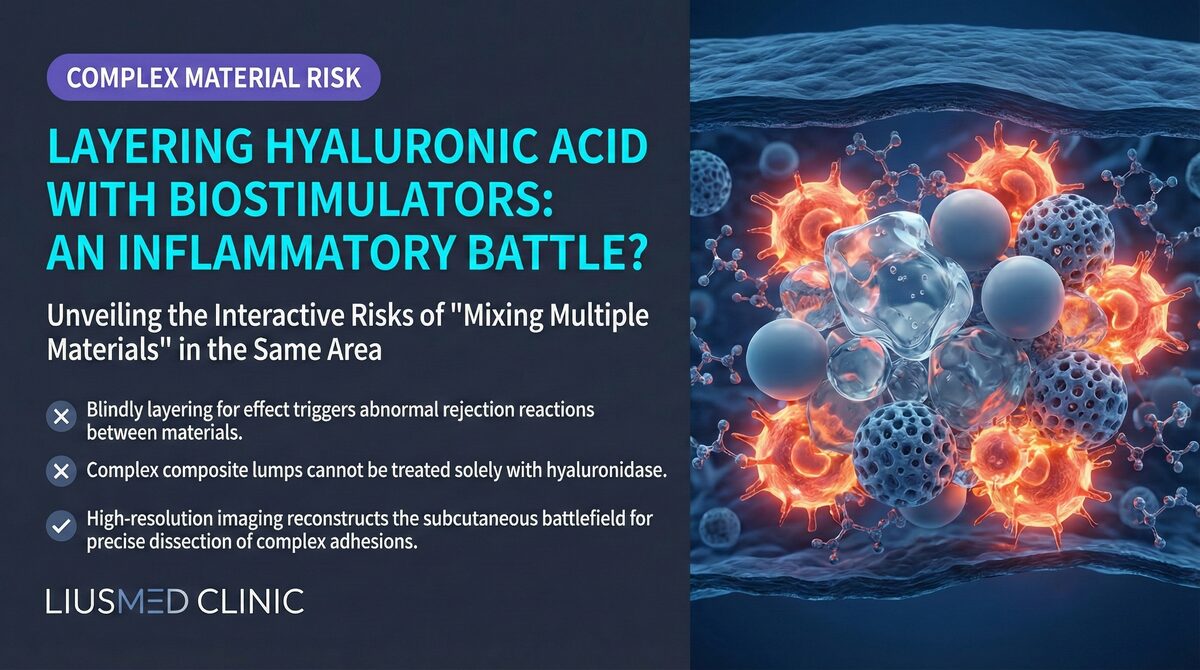
- Interact with newly injected fillers
- Be displaced to new positions when tissue is under pressure or trauma
Advice for Consumers
After understanding the persistence science of cross-linked HA, the following recommendations can help you make better decisions:
-
Do not assume HA will completely disappear. The labeled duration represents only the duration of "visible effects," not the disappearance of the substance.
-
Get an assessment before repeat injections. If you have received multiple HA injections over the past few years, an ultrasound assessment before your next injection can reveal cumulative residue status.
-
Hyaluronidase is not omnipotent. If you plan to "dissolve and redo," understand that enzymatic dissolution may not completely clear all residues.
-
Choose a physician with image-guidance capability. Whether for injection or repair, a physician who can see filler location under ultrasound can make more precise decisions.
If you have questions about persistent HA or want to know what remains in your tissue, FILLER REVISION provides ultrasound-based assessment that reveals the truth — because informed decisions require seeing what cross-linking chemistry left behind.
Key Insight: Cross-linking technology is the foundation that makes HA fillers work. But the same technology that makes fillers last also makes them harder for the body to clear and harder for enzymes to fully dissolve. Acknowledging this duality is the starting point for a truly scientific understanding of HA fillers.
Frequently Asked Questions
My HA filler was supposed to be absorbed in 6 to 18 months, so why can I still feel it years later?
Native hyaluronic acid has a half-life of only 1-2 days, but the chemical cross-linking that makes a product usable as filler also makes it resist the body's natural enzymatic breakdown. As a result, residues can persist for years beyond the labeled duration, which represents only the duration of visible effects, not the disappearance of the substance. This is a predictable consequence of the chemistry rather than a rare exception.
I had hyaluronidase injections but I can still feel residual filler. Why didn't it fully dissolve?
Hyaluronidase is not a magic eraser. High cross-link density, a fibrous capsule that forms around the filler over time, large bolus size, and sparse local blood flow can all reduce how effectively the enzyme works. For highly cross-linked, encapsulated, or large-bolus residues, enzymatic dissolution may be only partially effective or even completely ineffective, which is why some patients can still feel material after multiple injections.
Does where my filler was injected affect how likely it is to leave long-term residue?
Yes. Structural areas such as the nose bridge, chin, and cheekbones typically use highly cross-linked products, which are statistically more likely to have persistent residues detectable on ultrasound years after injection than the softer formulations used for areas like lips and tear troughs. The degree of cross-linking in your specific product influences how it responds to hyaluronidase and how likely it is to have formed residual deposits.
I want to dissolve old filler and inject new filler. Should I get checked first?
An ultrasound assessment before repeat injections is recommended, because if you have had multiple HA injections over the past few years it can reveal cumulative residues that you may assume have fully absorbed. High-resolution ultrasound can confirm whether old residues exist, assess their distribution, size, and degree of encapsulation, and determine whether they are causing current symptoms. Do not assume hyaluronidase will completely clear everything before you redo the area.
If hyaluronidase can't dissolve my residue, is there another way to remove it?
Yes. For encapsulated or highly cross-linked residues where enzymatic dissolution has limited effect, ultrasound-guided minimally invasive extraction can physically remove the residue directly, avoiding the uncertainty of repeated enzyme injections. It also avoids the risk that excessive hyaluronidase dissolves the native HA in surrounding normal tissue. The right path is chosen based on what ultrasound imaging shows about the specific material present; details are discussed case by case during consultation.