
Capsular Contracture After Filler
"The filler itself was fine at first — but over months the area grew tight, hard, and started to distort when I smiled." At FILLER REVISION, capsular contracture patients describe a slow tightening rather than a sudden lump. When the body walls off a filler or biostimulator deposit, it builds a fibrous capsule around it. Normally that capsule stays thin and soft — but in some people it thickens and contracts, squeezing the material into a firm, sometimes visibly distorted mass that pulls on the surrounding tissue. It can follow any long-lasting filler — HA, collagen stimulators (Sculptra, Ellansé, AestheFill), or permanent materials — and unlike fresh swelling, it does not settle with time, massage, or anti-inflammatories, because the problem is the contracted scar capsule, not active inflammation.
Common Symptoms
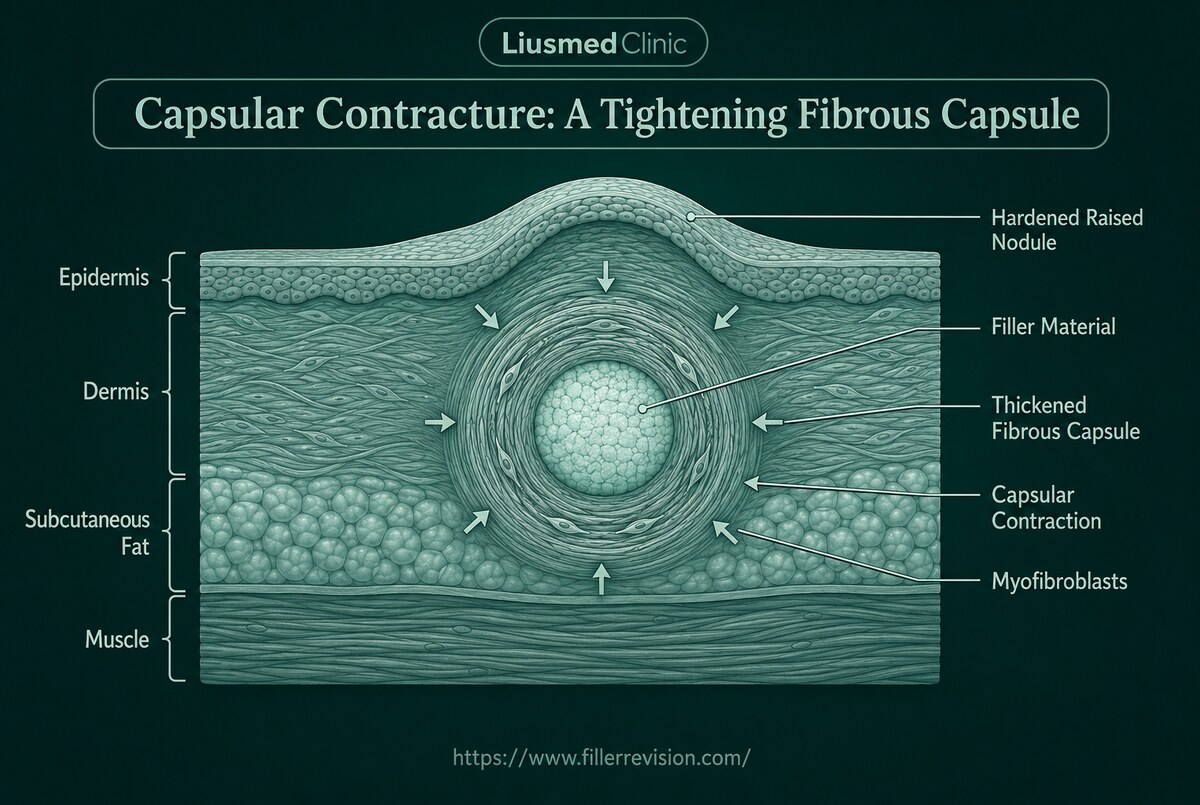
From Normal Encapsulation to a Contracting Scar
Encapsulation is a normal, protective response: the body surrounds any implanted material with a thin fibrous membrane. The problem begins when that membrane behaves like scar tissue and contracts. Myofibroblasts within the capsule generate tension and progressively tighten it, much like the capsular contracture long recognized around breast implants. The same biology can develop around facial filler — particularly biostimulators and permanent materials that persist for years and keep the foreign-body response active. As the capsule contracts, it compresses the deposit, increases its firmness, and tethers the overlying skin, which is why the distortion often becomes most obvious during movement and expression. Because the driver is a mature fibrous capsule rather than fluid swelling, the hardness is stable and does not fluctuate the way early inflammation does.
Why Traditional Treatments Fail
Why Massage, Steroids, and Dissolving Fall Short
The usual first-line measures target the wrong layer. Massage cannot stretch a mature, contracted capsule and may simply spread discomfort. Steroid injection calms inflammation but does not dissolve organized scar tissue, and repeated use thins the skin and atrophies the fat, sometimes adding a depression on top of the hardness. For HA, hyaluronidase can only reach gel that the enzyme can contact — material sealed inside a thick capsule is largely shielded, so dissolving attempts often disappoint. Biostimulators and permanent fillers have no dissolving agent at all. As long as the contracted capsule and the material inside it remain, the tightening tends to persist or slowly progress.
“Capsular contracture patients are often told their filler 'just needs time to soften' — but a contracted scar capsule doesn't soften on its own; it tends to tighten. The moment that changes everything is when I show them, on ultrasound, the firm rim of scar wrapped around the material and pulling on their skin. Once they see that the hardness is a structure, not swelling, it's clear why creams and massage never worked — and why releasing the capsule is what actually frees the tissue.”
Dr. LiuRelease the Capsule, Don't Just Soften the Surface
Ultrasound-Guided Pinhole Micro-Extraction
The hardness of capsular contracture is a structure — a contracted scar capsule wrapped around persisting material. You cannot massage or medicate a mature capsule into releasing. The result patients want — soft, mobile, even tissue — comes from removing the capsule and its contents, not from adding or suppressing.
The Tightness Is Scar, Not Swelling
At FILLER REVISION, capsular contracture patients have usually spent months on massage, creams, and steroids aimed at 'swelling' that was never swelling. The firmness is a contracted fibrous capsule, and it responds to release, not to suppression.
Why It Distorts With Expression
A contracted capsule tethers skin to the deposit beneath it. We map that capsule on ultrasound so the release targets exactly what is restricting movement — the reason the distortion shows most when you smile or speak.
A Clean, Even Result
Releasing the capsule and extracting the material cleanly — leaving the plane flat rather than ridged — is what restores natural contour and motion. The standard we hold is not just 'it's out,' but that the area moves and looks even afterward.
Ultrasound-Guided Capsule Release and Extraction
We treat the structure causing the problem: the contracted capsule and the material it encloses. High-resolution ultrasound maps the capsule's depth, thickness, and relationship to nerves and vessels before anything is done. Through a small entry point we release the fibrous capsule and remove the encased deposit, aiming to take out the material cleanly and leave the tissue plane flat rather than ridged. Where the capsule has tethered the skin, releasing it allows the area to move naturally again. The goal is not just removal but an even, untethered result that restores normal contour and expression.
Ultrasound Capsule Mapping
Pain-Controlled Local Anesthesia
Capsule Release
Clean Material Extraction
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
It is the same underlying biology — a fibrous capsule that contracts — applied to a much smaller deposit. The body walls off the material, and in some people that capsule thickens and tightens. The scale and the treatment differ, but the mechanism of a contracting scar capsule is shared, which is why simply softening the surface rarely helps.
A contracted capsule tethers the overlying skin to the firm deposit underneath. When the muscles move, the tethered area can't glide normally, so puckering or distortion becomes most visible with expression. Releasing the capsule is what restores natural movement, not adding more filler on top.
Hyaluronidase only works on gel it can physically contact. When HA is sealed inside a thick fibrous capsule, the enzyme is largely blocked, which is why repeated dissolving sessions can leave the hardness unchanged. Ultrasound lets us see whether the material is encapsulated and reach what the enzyme cannot.
Steroids reduce inflammation but do not break down a mature scar capsule. Short-term softening is sometimes seen, but the contracture usually returns once the effect fades, and repeated injections risk skin thinning and fat loss that can leave a dent next to the hardness.
Ultrasound distinguishes them. A contracted capsule shows a characteristic fibrous rim around a defined deposit, a granuloma shows active inflammatory tissue, and free filler looks different again. Mapping this before treatment determines the right approach and avoids unnecessary procedures.
The aim is a clean, even extraction that leaves the tissue plane flat rather than ridged, through a small entry point. Some volume the deposit occupied may need time to settle, and any restorative step is planned only after full healing and confirmation that the area is stable.
It is usually a delayed process, developing over months to years rather than days. Long-lasting biostimulators and permanent fillers, which keep the foreign-body response active, are more often involved than short-lived HA, though encapsulated HA can also contract.
Fresh swelling does settle with time — a mature contracted capsule generally does not. If an area has been progressively hardening or tightening for months despite massage and anti-inflammatories, waiting longer rarely changes the outcome, and ultrasound assessment is the practical next step.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then message us on Telegram with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your Telegram message, mention you posted in the FillerRescue forum.
Read next: how we actually handle it
Case-by-case decisions, written by Dr. Ta-Ju Liu
Encapsulation: Why Dissolvers Failed to Fix Your Filler Problem
Why your body builds a wall around filler that dissolvers cannot penetrate — and how ultrasound-guided extraction provides the root-cause solution.
Severe Tissue Adhesion and Fibrosis: How FILLER REVISION's Staged Approach Succeeds After Multiple Failed Procedures
A layered, progressive technique treats severe adhesion and fibrosis from repeated procedures, with gradual improvement where aggressive sessions fail.
References
- Lemperle G, et al. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009;123(6):1842-1863.
- Alijotas-Reig J, et al. Late-onset inflammatory adverse reactions related to soft tissue filler injections. Clin Rev Allergy Immunol. 2013;45(1):97-108.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.