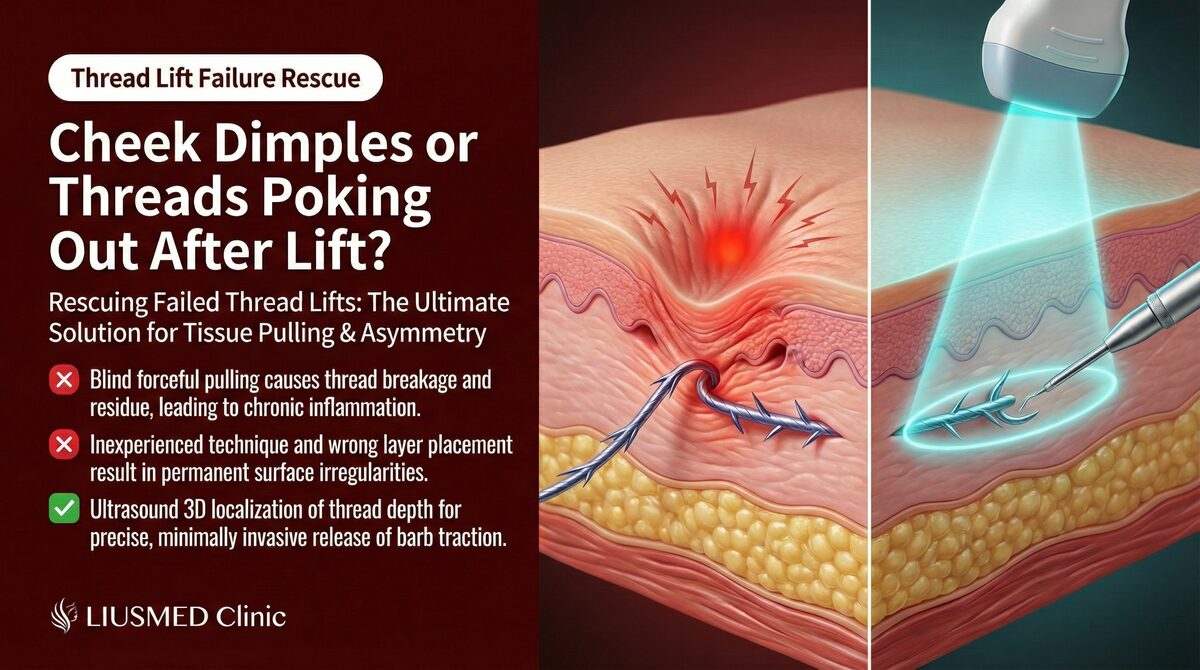
After a Thread Lift: Why Do Threads Come Through the Skin?
"I can feel the threads under my skin, and one end keeps poking through. My doctor says to wait for them to absorb, but it's been months and the inflammation keeps coming back." At FILLER REVISION, thread lift complications are among our most technically challenging cases because the threads are invisible beneath the skin — you can feel them, but no one can see exactly where they run without imaging. Patients arrive after months of recurring inflammation, repeated antibiotics, and the frustrating advice to "just wait for absorption" while threads protrude through the skin or trigger foreign body reactions. In our experience, ultrasound-guided localization and removal is the primary way to definitively resolve these complications.
Key Insight: At FILLER REVISION, we see this pattern regularly — thread lift materials come in many types, each with distinct complication profiles. The first step in managing thread lift complications is confirming the thread type, location, and current condition.
Common Thread Materials and Complication Comparison
Thread Type Characteristics
← Swipe to see more →
| Thread Type | Material | Absorption Time | Common Complications |
|---|---|---|---|
| PDO (Polydioxanone) threads | Polydioxanone | 6–8 months | Protrusion, infection, asymmetry |
| PLLA (Poly-L-Lactic Acid) threads | Poly-L-lactic acid | 12–18 months | Nodules, chronic inflammation |
| PCL (Polycaprolactone) threads | Polycaprolactone | 24–36 months | Foreign body reaction, palpability |
| Hybrid threads | PDO+PLLA combinations | Varies | Uneven absorption, local reactions |
Why Complications Occur
-
Thread Protrusion
- Insufficient placement depth: Threads positioned too close to the skin surface
- Thin skin: Higher risk in areas like the jawline and temples where skin is thinner
- Tissue tension: Facial movements (chewing, expressions) place continuous stress on threads
- Improper thread end management: Thread ends not adequately anchored in deep tissue
-
Recurrent Inflammation
- Biofilm formation on thread surfaces
- Foreign body reaction continually activating the immune system
- Chronic low-grade infection around the thread
- Degradation products from the absorption process causing irritation
-
Palpable Threads
- Inappropriate placement layer
- Tissue atrophy causing the thread to shift relatively closer to the surface
- Thread migration to a shallower plane
- Uneven collagen encapsulation
Key Insight: Timing matters in thread complication management. Protrusion or inflammation detected early is typically easier to manage than cases left for months. If a thread has partially protruded through the skin, do not attempt to push it back or pull it out yourself.
The Role of Ultrasound (Ultrasonography) in Thread Lift Complications
Why Ultrasound Is Needed
The greatest challenge in managing thread lift complications is invisibility. The thread's path through tissue, its depth, and its relationship to surrounding structures cannot be adequately assessed through palpation and visual inspection alone.
← Swipe to see more →
| Ultrasound Capability | Clinical Value |
|---|---|
| Thread localization | Confirm the precise course and depth of each thread |
| Protrusion assessment | Determine whether protrusion is a local issue or entire thread displacement |
| Inflammation mapping | Evaluate the degree of tissue reaction around the thread |
| Vascular identification | Avoid important facial blood vessels |
| Multi-thread tracking | Identify each thread individually in cases with multiple placements |
Ultrasound Appearance of Different Threads
← Swipe to see more →
| Thread Type | Ultrasound Appearance | Identifying Features |
|---|---|---|
| PDO threads | Linear hyperechoic signal | Clear linear structure |
| PLLA threads | Hyperechoic with surrounding hypoechoic halo | More pronounced surrounding tissue reaction |
| PCL threads | Hyperechoic linear structure | Well-defined boundary with surrounding tissue |
| Cog threads | Serrated hyperechoic pattern | Barb structures may be visible |
Ultrasound-Guided Thread Removal
Indications
Ultrasound-guided thread removal is recommended when:
- Thread protrusion through the skin recurs repeatedly
- Persistent inflammation around a thread continues for 4–6 weeks or longer
- Palpable threads cause discomfort or affect appearance
- Chronic infection from the thread responds poorly to antibiotics
- The patient strongly desires thread removal
The Removal Process
Assessment Phase
- History confirmation: Thread type, placement date, performing practitioner, symptom timeline
- Ultrasound scan: Trace the course, depth, and skin proximity of all threads
- Surrounding tissue evaluation: Inflammation degree, infection signs, vascular positions
Surgical Phase
- Local anesthesia
- Ultrasound-guided identification of the target thread
- Entry through a micro-incision (1–2mm) or the existing protrusion site
- Under continuous ultrasound monitoring, separate and extract the thread along its course
- Confirm complete thread removal or manage remaining segments
- Ultrasound verification of extraction result
Post-Procedure Care
- Clean wound care
- Ice application within 48 hours to reduce swelling
- Avoid excessive facial movements for one week
- Follow-up appointment at one week
Challenges and Expectations
← Swipe to see more →
| Scenario | Removal Difficulty | Expected Outcome |
|---|---|---|
| Partially protruding thread | Lower | Can be guided out through the protrusion site |
| Deep intact thread | Moderate | Requires precise ultrasound localization for extraction |
| Cog thread (barbed) | Higher | Barbs may be entangled with tissue; careful separation needed |
| Multiple threads | Moderate to high | Sequential removal; may require staged sessions |
| Peri-thread abscess | Lower | Remove thread and drain simultaneously |
| Partially absorbed remnant | Moderate | Remove symptomatic remaining segments |
When Waiting for Absorption Never Resolves the Problem: The FILLER REVISION Approach
The most common advice thread lift complication patients receive is "wait — the threads will absorb." While technically true for PDO threads (6-8 months) and eventually for PLLA and PCL threads, this advice ignores a critical reality: if a thread is causing protrusion, inflammation, or infection now, the damage continues accumulating while you wait. Biofilm may form on the thread surface, chronic inflammation may produce fibrosis, and protruding thread ends create entry points for bacteria. At FILLER REVISION, ultrasound localization transforms thread removal from a blind procedure into a precise one. We trace each thread's exact course, depth, and relationship to surrounding vessels and nerves before extraction. For barbed (cog) threads entangled with tissue, this real-time guidance is essential for safe separation and complete removal. The result is definitive resolution of the complication rather than months of suppressive antibiotics and hopeful waiting.
Inflammation Without Protrusion: What to Do?
Conservative Treatment Options
Not every thread lift complication requires thread removal. Conservative management may be appropriate in the following situations:
← Swipe to see more →
| Scenario | Recommended Approach |
|---|---|
| Early mild swelling (<2 weeks post-procedure) | Observation, ice, oral anti-inflammatory medication |
| Mild localized tenderness | Observe for 4–6 weeks; most resolve spontaneously |
| Superficial infection | Oral or topical antibiotics |
| Deep infection | Oral antibiotics + ultrasound monitoring |
When to Transition From Conservative to Removal
- No improvement after 2–4 weeks of antibiotic therapy
- Recurrent inflammatory episodes
- Formation of a definite abscess
- Thread beginning to protrude
- Patient unable to tolerate continued discomfort
Preventing Thread Lift Complications
Pre-Procedure Evaluation
- Skin thickness assessment: Extra caution in thin-skinned areas
- History of allergies and foreign body reactions
- Understanding of thread type and quality
- Selection of an experienced practitioner
Post-Procedure Guidelines
- Avoid wide facial movements for 48–72 hours post-procedure
- Avoid sleeping on the treated side
- Attend scheduled follow-up appointments
- Seek immediate medical attention if you notice redness, increasing pain, or the sensation of a thread end
Do Not Let Thread Problems Affect Your Daily Life
If you've already tried treatment for thread lift complications without success — or been told to simply wait for absorption while symptoms persist — FILLER REVISION specializes in exactly these cases. Our ultrasound-guided thread removal provides definitive resolution.
Further reading:
- Minimally Invasive Filler Lump Extraction Technique
- The Filler Repair Evaluation Process
- Why Dissolving Enzymes Fail When Capsules Form
Frequently Asked Questions
My doctor told me to just wait for the threads to absorb, but the inflammation keeps coming back. Is waiting the right approach?
Waiting is only reasonable when a thread is not actively causing problems. If a thread is causing protrusion, inflammation, or infection now, the damage continues accumulating while you wait — biofilm may form on the thread surface, chronic inflammation may produce fibrosis, and protruding ends create entry points for bacteria. While PDO threads do absorb in 6–8 months and PLLA/PCL eventually too, this advice ignores the ongoing tissue damage during that wait. When inflammation keeps recurring, active intervention rather than continued waiting is usually warranted.
A thread end is poking through my skin. Can I push it back in or pull it out myself?
No. If a thread has partially protruded through the skin, do not attempt to push it back or pull it out yourself. The thread's full course and depth are invisible beneath the skin, and pulling blindly risks tissue damage. Timing matters too — protrusion detected early is typically easier to manage than cases left for months. If you notice redness, increasing pain, or the sensation of a thread end, seek medical attention promptly.
Why is ultrasound needed to remove threads — can't the doctor just locate them by feel?
The greatest challenge with thread complications is invisibility — the threads are hidden beneath the skin, so you might feel them but no one can see exactly where they run without imaging. The thread's path, its depth, and its relationship to surrounding structures cannot be adequately assessed through palpation and visual inspection alone. Ultrasound traces each thread's exact course, depth, and relationship to nearby vessels before extraction, and it helps avoid important facial blood vessels. This is what transforms removal from a blind procedure into a precise one.
Does every thread lift complication need the thread removed?
No. Not all thread complications require removal. Early mild swelling within about two weeks of the procedure may be managed with observation, ice, and oral anti-inflammatory medication, and mild localized tenderness often resolves spontaneously over 4–6 weeks. Superficial or deep infection may be treated with antibiotics, sometimes alongside ultrasound monitoring. Removal becomes the recommended path when inflammation recurs, an abscess forms, a thread begins to protrude, antibiotics don't help after 2–4 weeks, or the discomfort becomes intolerable.
What is thread removal actually like — is it a major operation?
It is a minimally invasive procedure. The thread is reached either through a 1–2mm micro-incision or the existing protrusion site, performed under local anesthesia, with the doctor in real-time communication with you throughout. Under continuous ultrasound monitoring, the thread is separated and extracted along its course, then ultrasound confirms the result. Afterward, wound care, ice within 48 hours, avoiding excessive facial movements for a week, and a one-week follow-up are advised. Note that minimally invasive does not mean painless, and the difficulty varies — barbed (cog) threads or multiple threads can be more involved and may need staged sessions.
After a thread lift, what warning signs mean I should see a doctor right away?
Seek immediate medical attention if you notice redness, increasing pain, or the sensation of a thread end. For the first 48–72 hours, avoid wide facial movements and avoid sleeping on the treated side, and attend your scheduled follow-up appointments. Persistent inflammation around a thread lasting 4–6 weeks or longer, recurrent inflammatory episodes, or a thread that starts to protrude are also signs that warrant evaluation rather than continued waiting.
About the Author
Dr. Ta-Ju Liu
- Current Position: Director, Liusmed Clinic
- Specialties: Minimally invasive surgery, filler complication repair, thread lifting, ultrasound-guided extraction
- Experience: 15+ years of clinical minimally invasive surgery; over 10,000 successful cases
- Philosophy: "The challenge with thread complications is that the threads are hidden beneath the skin — you might feel them, but you cannot see them. Ultrasound becomes our eyes, making the removal process safer and more precise."