Introduction
"My face looks like a mask. I've tried dissolving some of the filler, but it didn't bring back my natural expressions." At FILLER REVISION, Facial Overfilled Syndrome is one of our core specializations. Most FOS (Facial Overfilled Syndrome) patients who reach us have already attempted partial dissolution or other treatments that addressed volume but failed to restore natural facial dynamics. This authoritative guideline is based on the latest medical literature, clinical evidence, and FILLER REVISION's extensive experience treating complex FOS cases.
What is FOS?
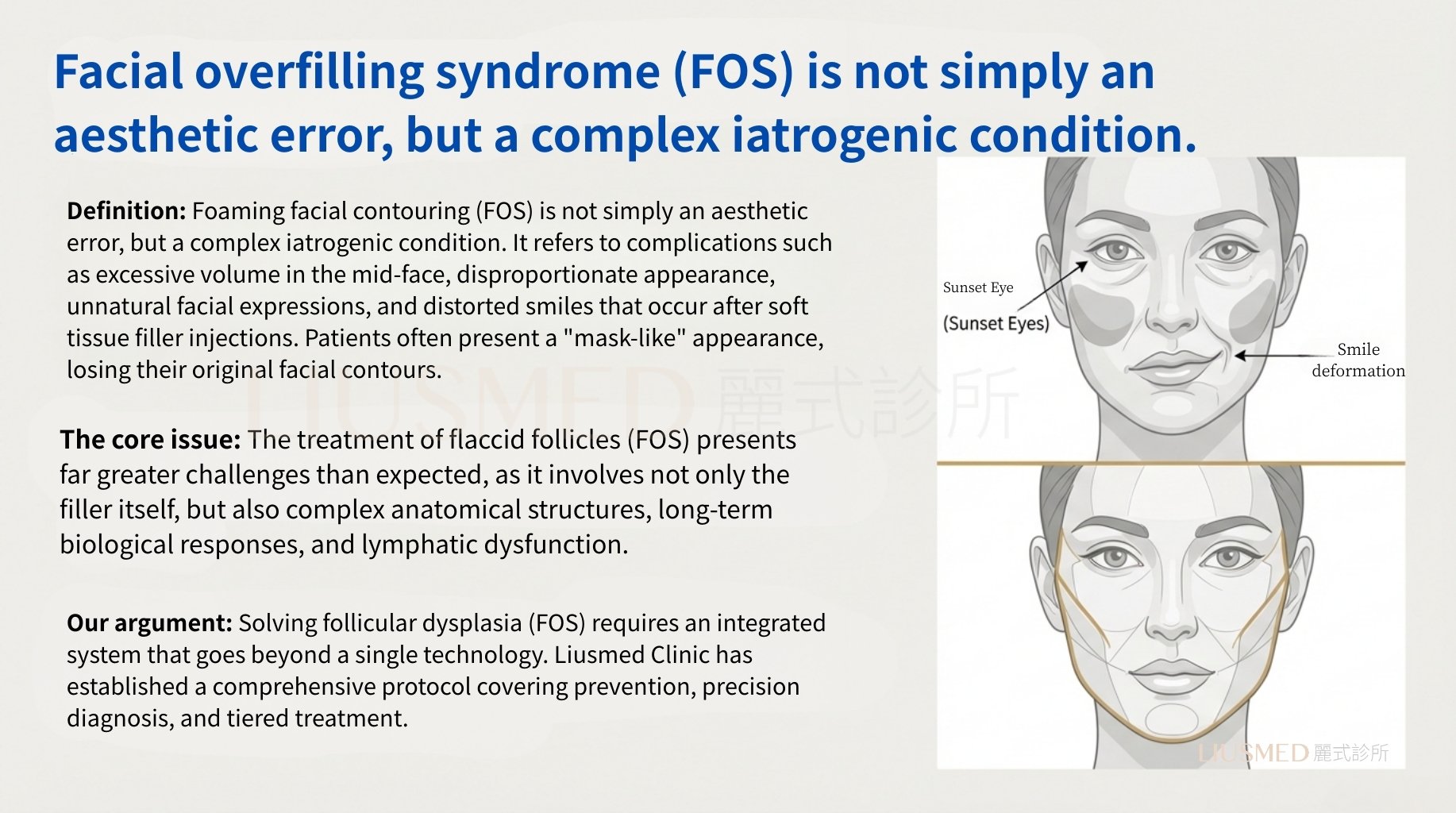
FOS is not simply an aesthetic mistake—it is a complex iatrogenic condition.
It refers to complications following soft tissue filler injections, presenting as excessive mid-face volume, disproportionate features, unnatural expressions, and smile distortion. Patients often exhibit a "mask-like" appearance with loss of natural facial contours.
The Core Problem
The treatment challenge of FOS far exceeds expectations because it involves not only the filler material itself but also:
- Complex anatomical structures
- Long-term biological reactions
- Lymphatic dysfunction
Our Position
Resolving FOS requires an integrated system that transcends single techniques.
Li-Shi Clinic has established a comprehensive guideline covering prevention, precision diagnosis, and tiered treatment.
Root Causes of FOS
Cause One: The Extremely Complex Anatomy of the Mid-Face
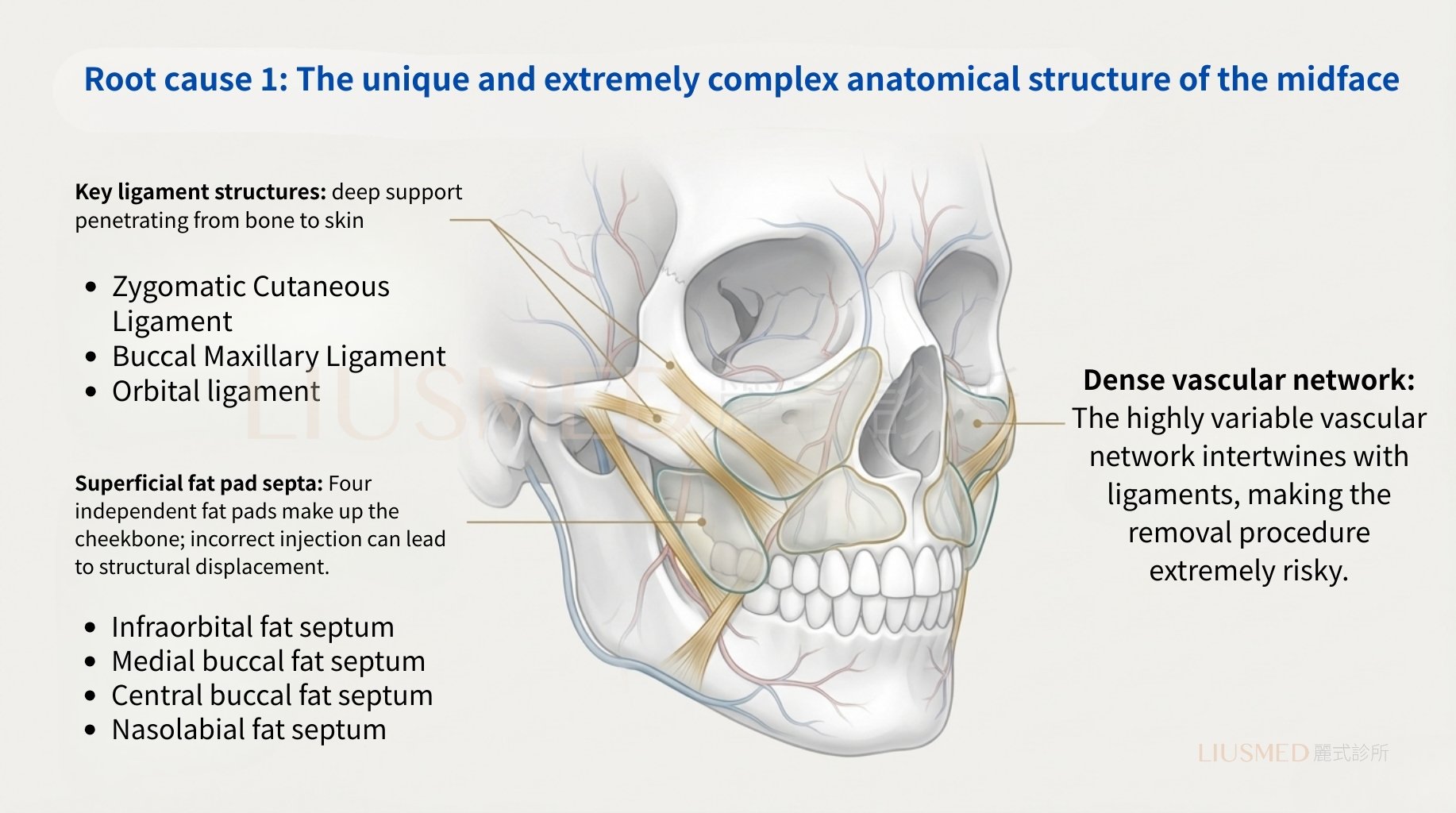
Key Ligamentous Structures
Deep support structures that penetrate from bone to skin, including:
- Cutaneous ligaments
- Zygomatic-maxillary ligaments
- Orbital ligaments
Superficial Fat Pad Compartments
Four independent fat pads form the malar region:
- Infraorbital fat compartment
- Medial cheek fat compartment
- Middle cheek fat compartment
- Nasolabial fat compartment
Incorrect injection can cause structural displacement.
Dense Vascular Network
Highly variable vascular networks interwoven with ligaments make removal procedures extremely risky.
Cause Two: Overlooked Pathological Mechanisms
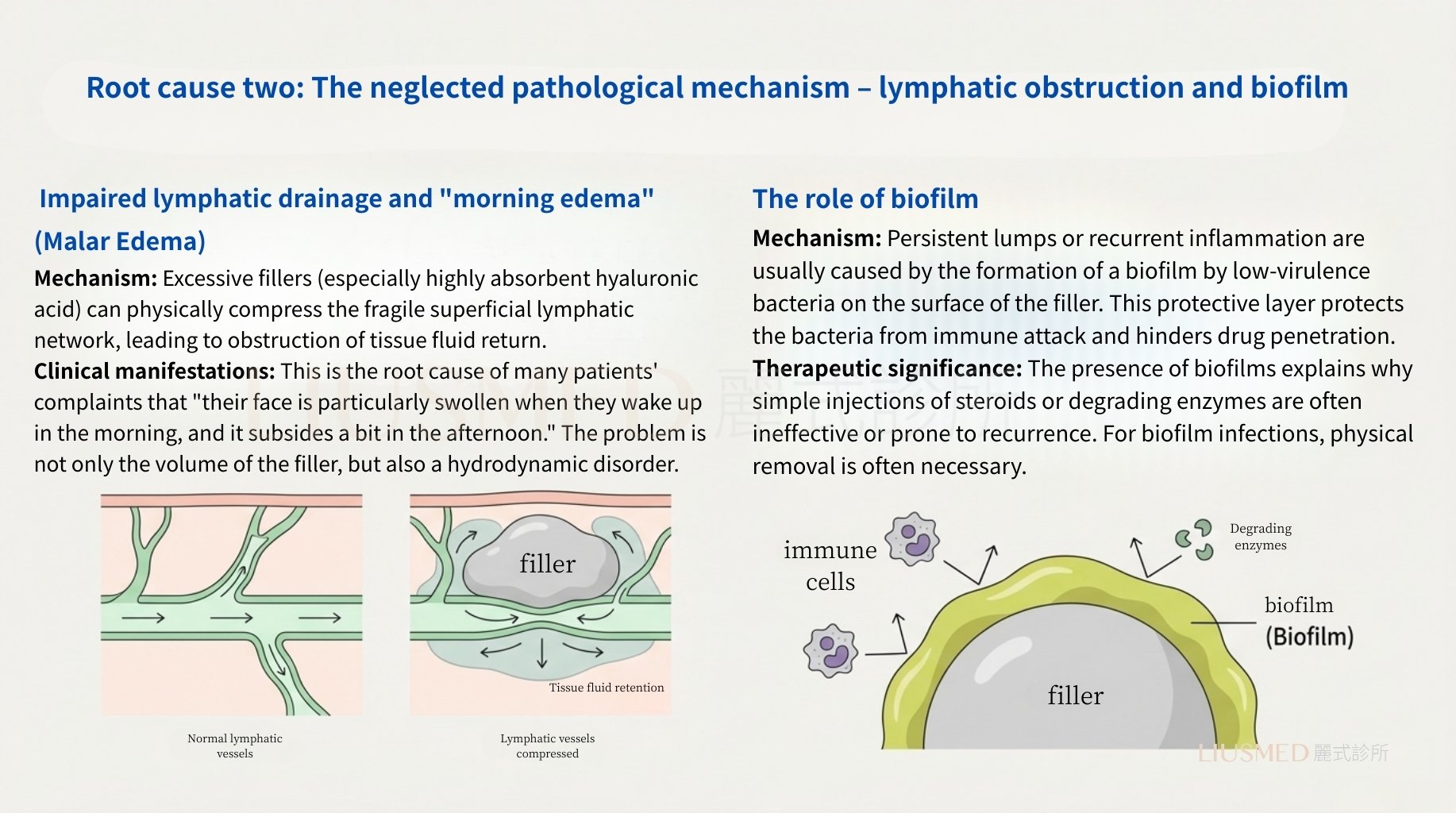
Lymphatic Obstruction and "Morning Edema"
Mechanism: Excessive filler (especially highly hydrophilic hyaluronic acid) physically compresses the fragile superficial lymphatic network, obstructing tissue fluid drainage.
Clinical Presentation: This is the root cause of many patients' complaints of "face being particularly swollen in the morning, improving by afternoon." The problem is not just filler volume but fluid dynamics disruption.
The Role of Biofilm
Mechanism: Long-standing nodules or recurrent inflammation are often caused by low-virulence bacteria forming biofilm on the filler surface. This protective layer shields bacteria from immune attack and prevents drug penetration.
Treatment Implications: The presence of biofilm explains why steroid or enzyme injections alone are often ineffective or lead to recurrence. For biofilm infections, physical removal is often necessary.
Clinical Diagnosis
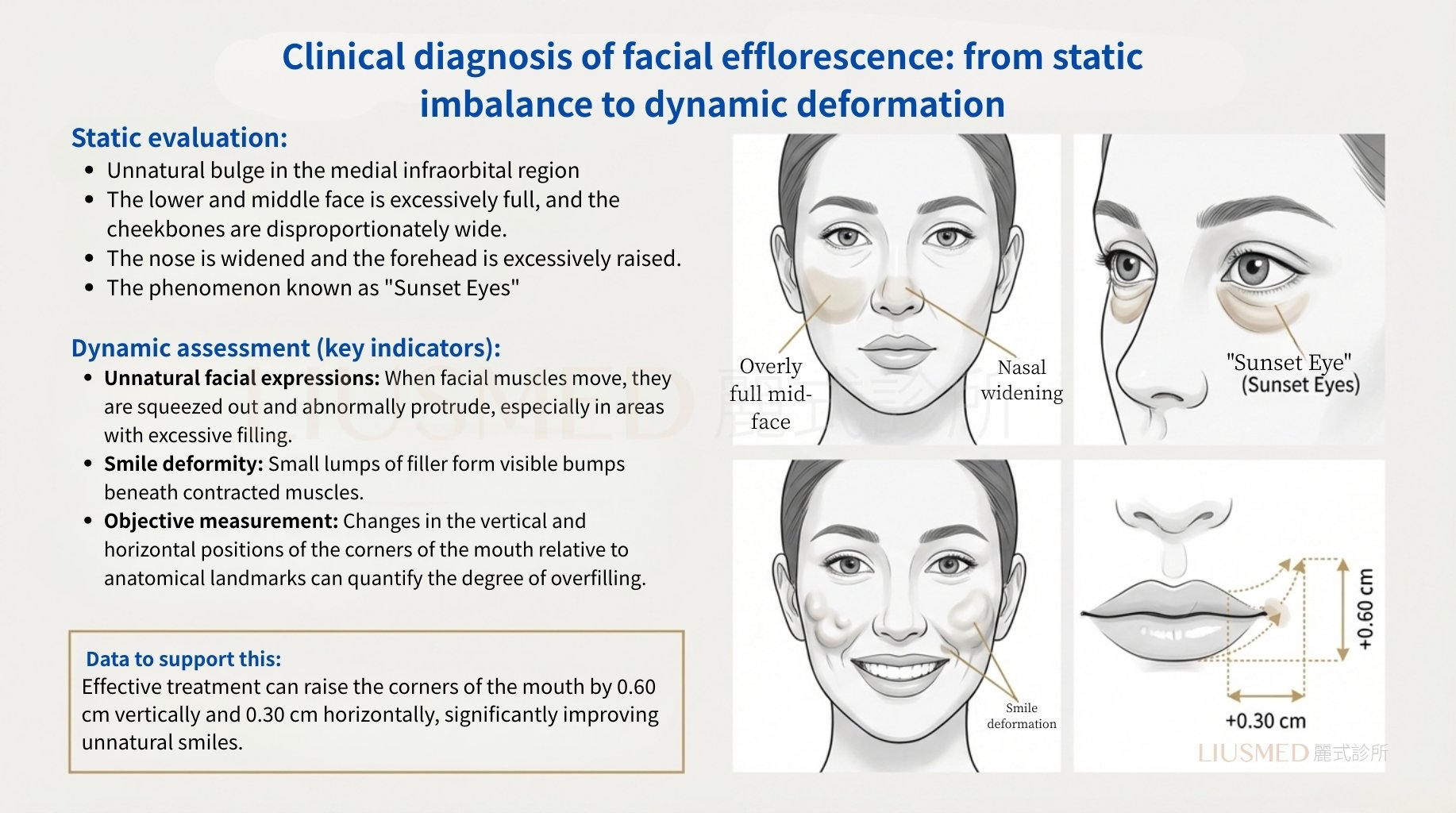
Static Assessment
- Topographical changes in the infraorbital-medial region
- Excessive lower mid-face fullness with disproportionate zygomatic arch widening
- Nasal widening and excessive forehead projection
- "Sunset Eyes" phenomenon
Dynamic Assessment (Key Indicators)
← Swipe to see more →
| Indicator | Description |
|---|---|
| Unnatural expressions | Overfilled areas become most apparent during facial muscle activity |
| Smile distortion | Small chunks of filler form visible bulges beneath contracting muscles |
| Objective measurements | Changes in oral commissure vertical and horizontal positions relative to anatomical landmarks |
Key Insight: At FILLER REVISION, we see this pattern regularly — effective treatment can elevate the oral commissure by 0.60 cm vertically and 0.30 cm horizontally, significantly improving unnatural smiles. Dynamic assessment during facial expressions is critical because FOS becomes most apparent during movement, not at rest.
The Current Treatment Dilemma
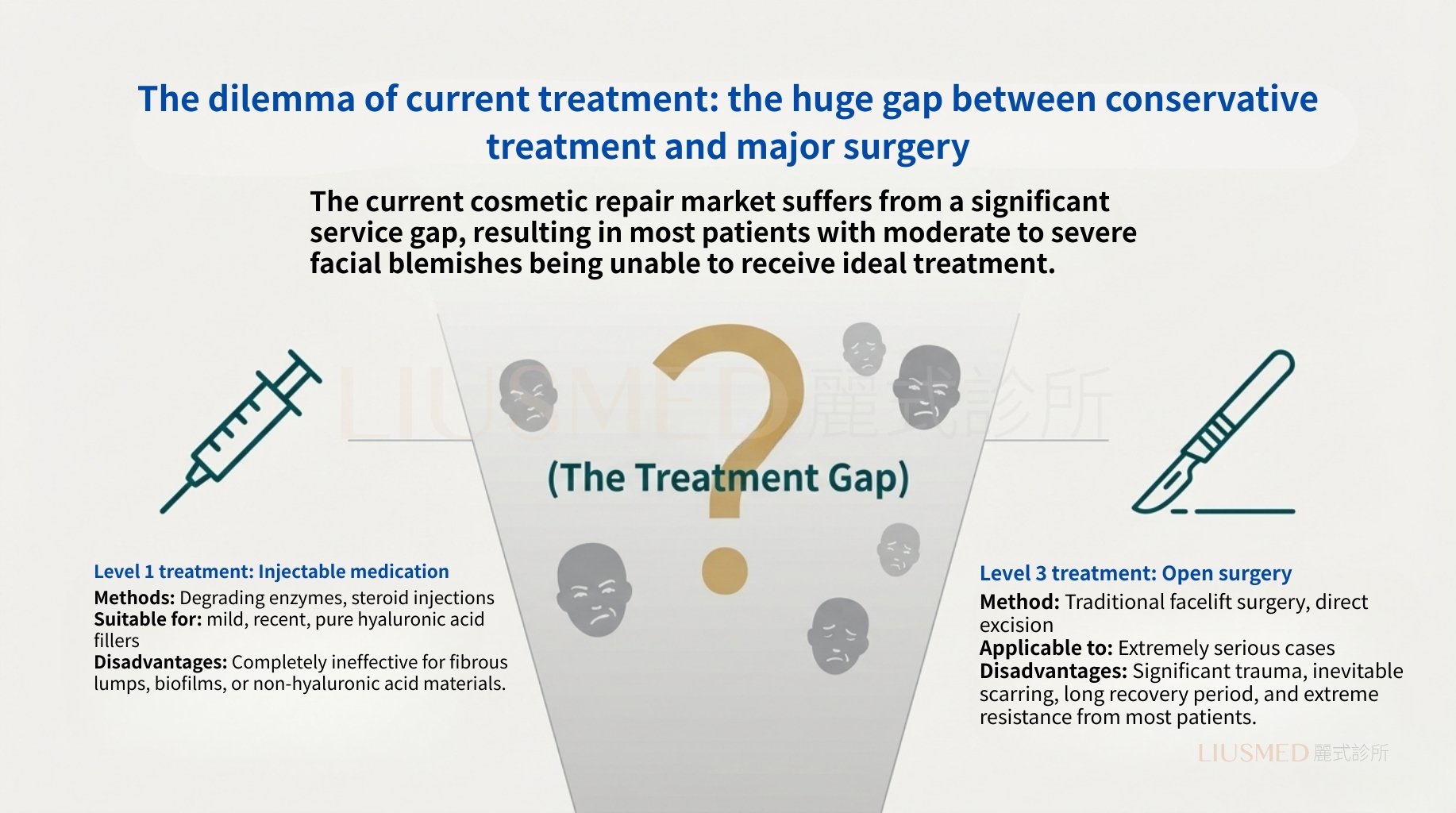
The current aesthetic repair market has a significant Treatment Gap, leaving most moderate to severe FOS patients without ideal treatment options.
Level 1 Treatment: Drug Injection
← Swipe to see more →
| Method | Limitations |
|---|---|
| Hyaluronidase | Ineffective for fibrotic nodules |
| Steroid injection | Completely ineffective for biofilm or non-HA (Hyaluronic Acid) materials |
Level 3 Treatment: Open Surgery
← Swipe to see more →
| Method | Limitations |
|---|---|
| Traditional facelift | Major trauma, inevitable scarring |
| Direct excision | Long recovery, most patients strongly resist |
A huge treatment vacuum exists between Level 1 and Level 3.
The Li-Shi FOS Treatment Guideline
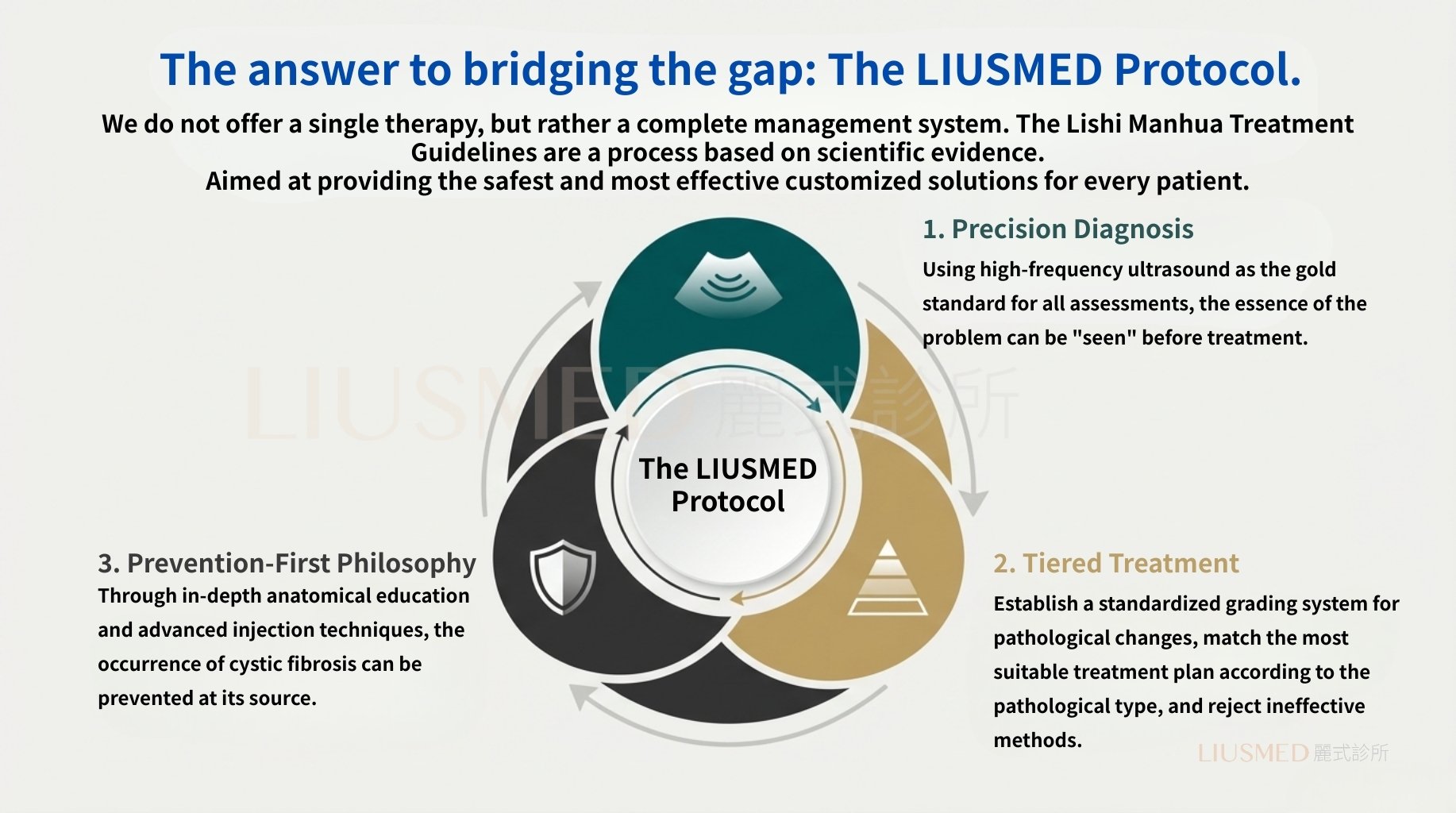
Core Philosophy
We don't offer a single therapy—we provide a complete management system. The Li-Shi FOS Treatment Guideline is an evidence-based closed-loop process.
Three Pillars
- Precision Diagnosis: High-frequency ultrasound as the gold standard for all assessments, "seeing" the problem before treatment
- Tiered Treatment: Standardized FOS classification system matching pathology types to optimal treatment protocols
- Prevention First: Preventing FOS at the source through deep anatomical education and advanced injection techniques
Guideline Pillar One: High-Frequency Ultrasound (Ultrasonography)
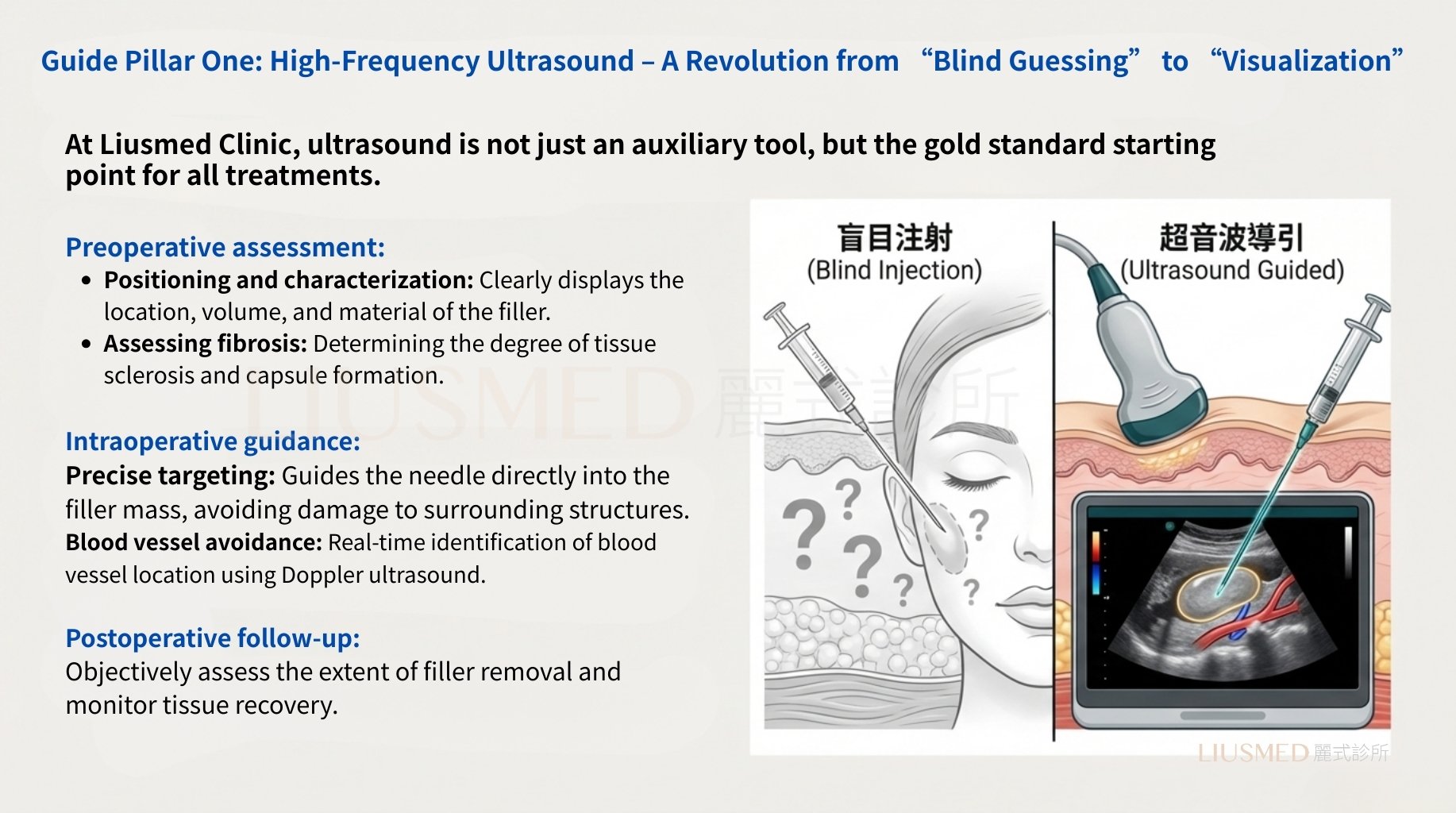
At Li-Shi Clinic, ultrasound is not just an auxiliary tool—it is the gold standard starting point for all treatments.
Pre-operative Assessment
- Localization and characterization: Clear visualization of filler location, volume, and material
- Fibrosis degree evaluation
Intra-operative Guidance
- Precision targeting: Guiding needles directly into masses
- Vascular avoidance: Real-time Doppler vessel identification
Post-operative Follow-up
- Objective assessment of removal degree
- Recovery monitoring
Guideline Pillar Two: FOS Classification and Treatment Protocol
Providing Precise Solutions for Complex Problems
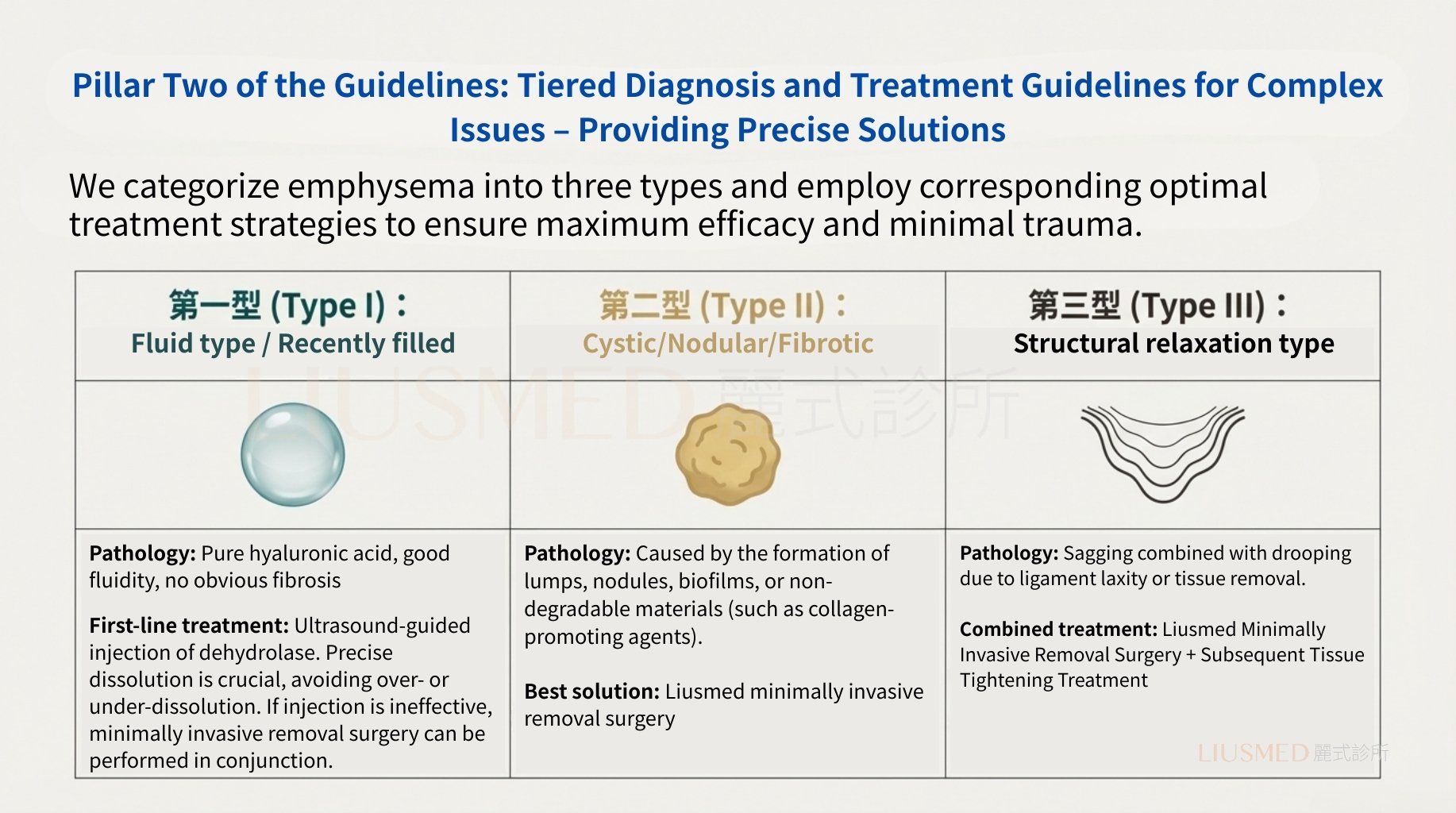
We classify FOS into three types with corresponding optimal treatment strategies, ensuring maximum efficacy with minimal trauma.
Type I: Fluid Type / Recent Filling
← Swipe to see more →
| Item | Description |
|---|---|
| Pathology | Pure hyaluronic acid, good fluidity, no significant fibrosis |
| Primary Treatment | Ultrasound-guided enzyme injection. Precise dissolution, avoiding over- or under-treatment. When injection is ineffective, minimally invasive removal can be combined |
Type II: Encapsulated / Nodular / Fibrotic Type
← Swipe to see more →
| Item | Description |
|---|---|
| Pathology | Formed nodules, masses, biofilm, or caused by non-degradable materials (e.g., collagen stimulators) |
| Best Solution | Li-Shi Minimally Invasive Removal |
Type III: Structural Laxity Type
← Swipe to see more →
| Item | Description |
|---|---|
| Pathology | FOS combined with sagging due to ligament laxity or post-removal tissue descent |
| Combined Treatment | Li-Shi Minimally Invasive Removal + subsequent tissue tightening treatment |
Gold Standard Technique: Li-Shi Minimally Invasive FOS Removal
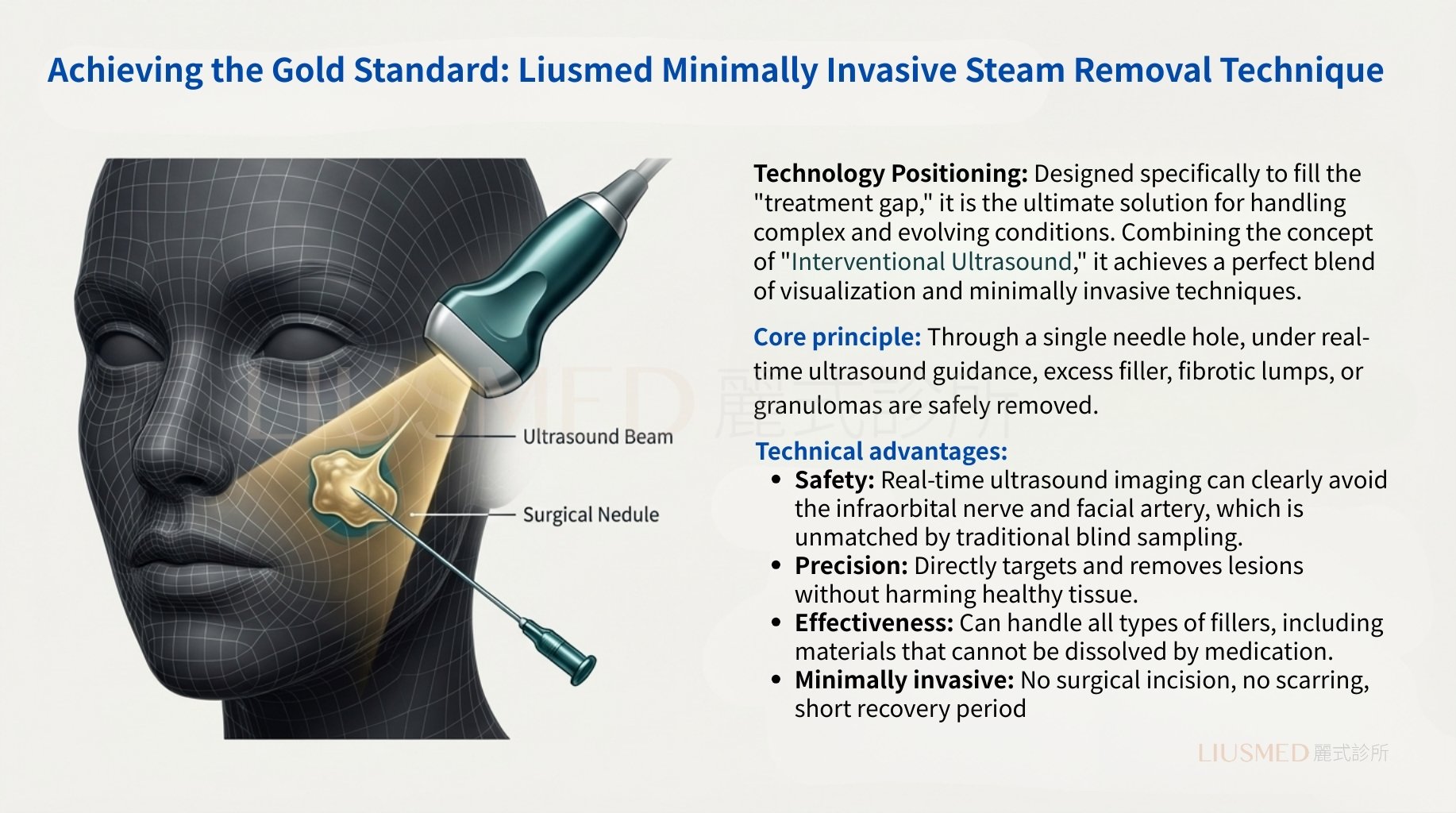
Technical Positioning
Designed specifically to bridge the "Treatment Gap," this is the ultimate solution for complex FOS. Combining "interventional ultrasound" concepts, it achieves the perfect integration of visualization and minimal invasiveness.
Core Principle
Through a single needle puncture, under real-time ultrasound guidance, safely remove excessive filler, fibrotic masses, or granulomas.
Technical Advantages
← Swipe to see more →
| Advantage | Description |
|---|---|
| Safety | Clear avoidance of infraorbital nerve and facial artery |
| Precision | Direct lesion-targeted destruction and removal, preserving healthy tissue |
| Efficacy | Can handle materials that drugs cannot dissolve |
| Minimal Invasiveness | No surgical incision, no scarring, extremely short recovery |
When Dissolution Alone Cannot Restore Natural Expressions: The FILLER REVISION Approach
Most FOS patients who arrive at FILLER REVISION have already tried partial dissolution — hyaluronidase to reduce volume in specific areas. While this can help with Type I fluid-type FOS, it consistently falls short for moderate to severe cases. The reason is that FOS involves not just excess filler volume but fibrotic changes, lymphatic obstruction, and structural displacement that enzymatic dissolution cannot reverse. At FILLER REVISION, our tiered approach matches the specific pathology to the optimal treatment: ultrasound-guided dissolution for fluid-type deposits, minimally invasive extraction for encapsulated and fibrotic material, and combined protocols with tissue tightening for structural laxity cases. This systematic classification is what separates effective FOS treatment from the trial-and-error approach that leaves patients cycling through partial improvements.
Technical Analysis: Precision Dissection and Removal
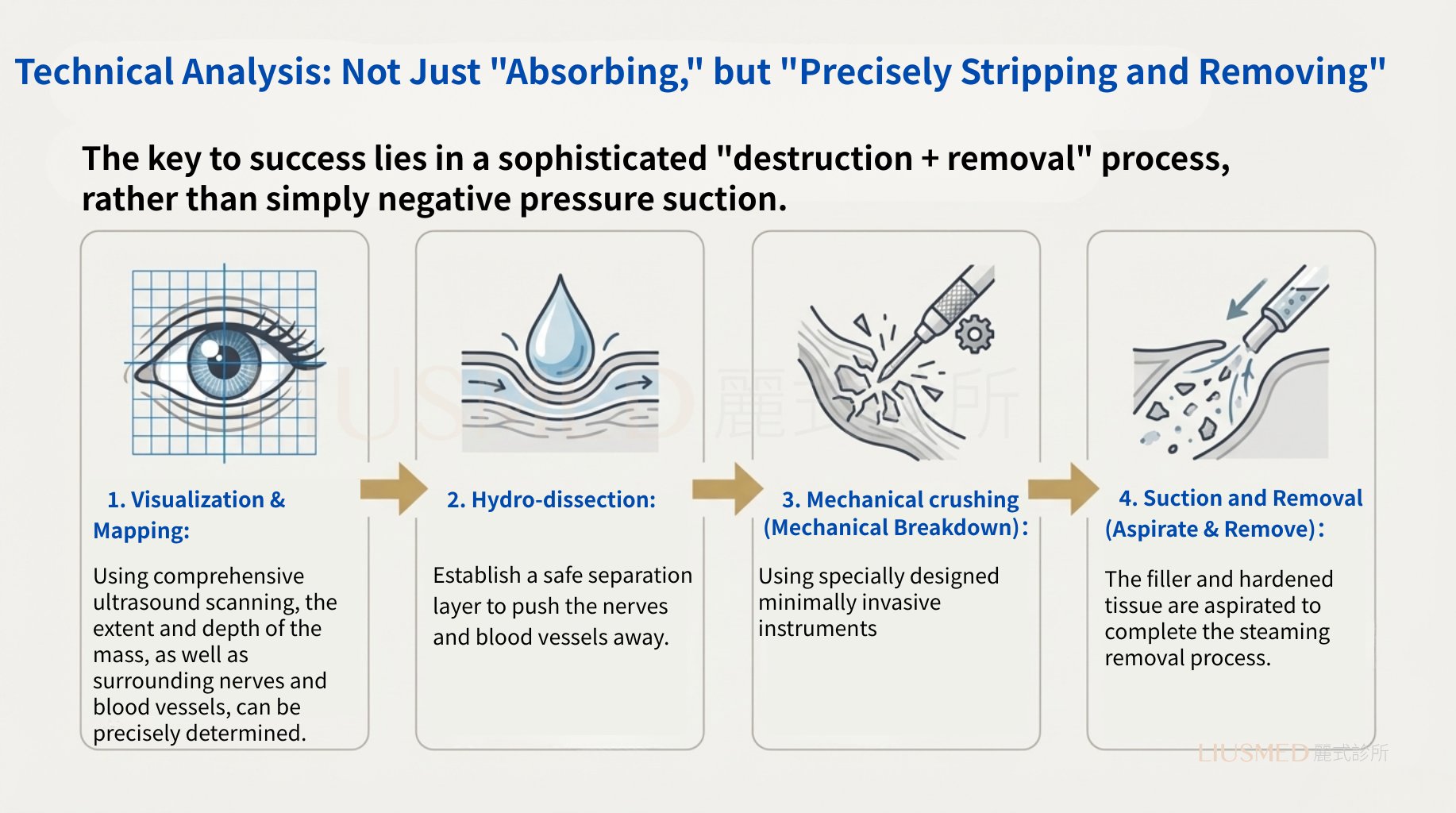
Not Just "Aspiration," But "Precision Dissection and Removal"
The key to success lies in a precise "breakdown + removal" protocol, not simple negative pressure suction.
1. Visualize & Map
Comprehensive ultrasound scanning to precisely locate mass extent, depth, and surrounding neurovascular structures
2. Micro-dissection
Creating a safe separation plane, pushing nerves and vessels away
3. Mechanical Breakdown
Using minimally invasive instruments
4. Aspirate & Remove
Extracting filler and hardened tissue, completing FOS removal
"Addition After Subtraction": Post-Removal Cavity Management and Tissue Rebalancing
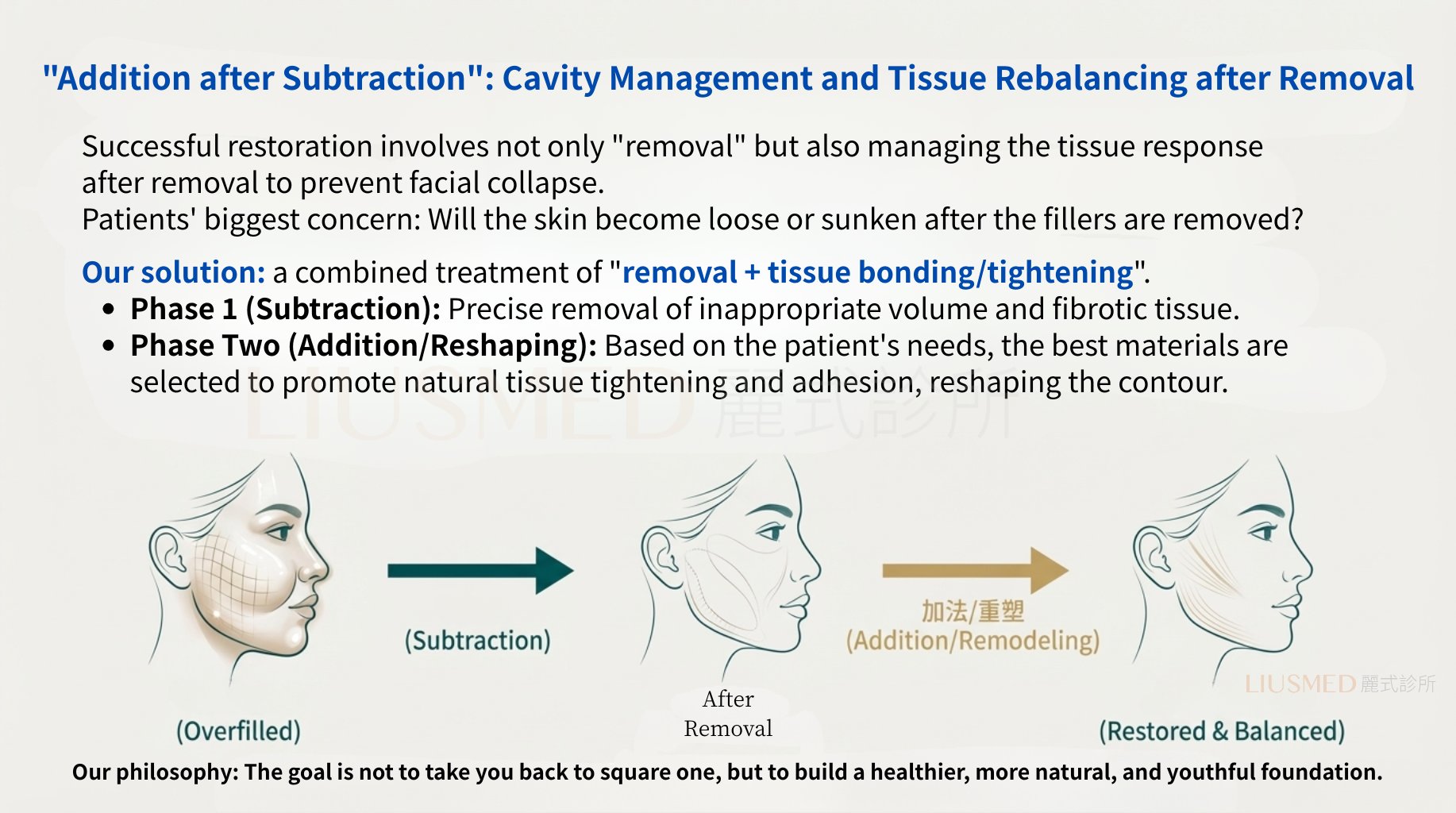
Successful repair is not just about "removal"—it's about managing post-removal tissue response to prevent facial collapse.
Patient's Greatest Concern
Will the skin become loose or sunken after filler removal?
Our Solution
"Removal + Tissue Adaptation/Tightening" Combined Protocol
Phase One (Subtraction)
Precise removal of inappropriate volume and fibrotic tissue
Phase Two (Addition/Reshaping)
Based on patient needs, selecting optimal materials to promote natural tissue tightening and contour reshaping
Our Philosophy: The goal is not to return you to the starting point, but to establish a healthier, more natural foundation for rejuvenation.
Guideline Pillar Three: Prevention Over Treatment
Establishing New Standards of Excellence in Injection
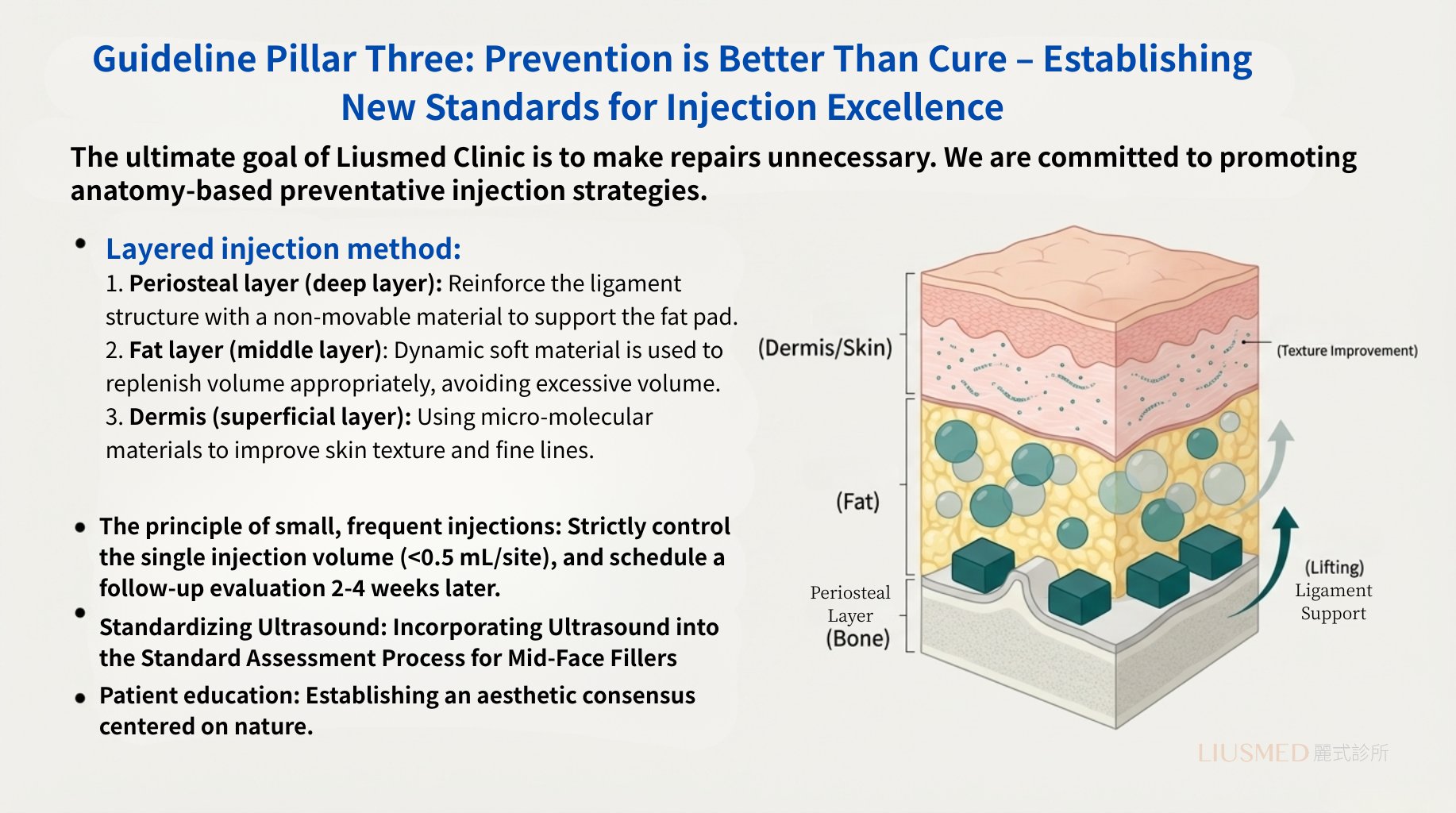
Li-Shi Clinic's ultimate goal is to make repair unnecessary. We are committed to promoting anatomy-based preventive injection strategies.
Layered Injection Approach
← Swipe to see more →
| Layer | Material | Purpose |
|---|---|---|
| Periosteal Layer (Deep) | Non-migrating materials | Ligament structure reinforcement, fat pad support |
| Fat Layer (Middle) | Dynamic soft materials | Moderate volume supplementation, avoiding excess |
| Dermal Layer (Superficial) | Micro-molecular materials | Skin quality and fine line improvement |
Implementation Principles
- Less is More: Strict control of single injection volume (<0.5 mL/site), with 2-4 week follow-up evaluation
- Ultrasound Standardization: Incorporating ultrasound into standard mid-face filling assessment protocols
- Patient Education: Establishing aesthetic consensus centered on natural results
Li-Shi's Core Philosophy
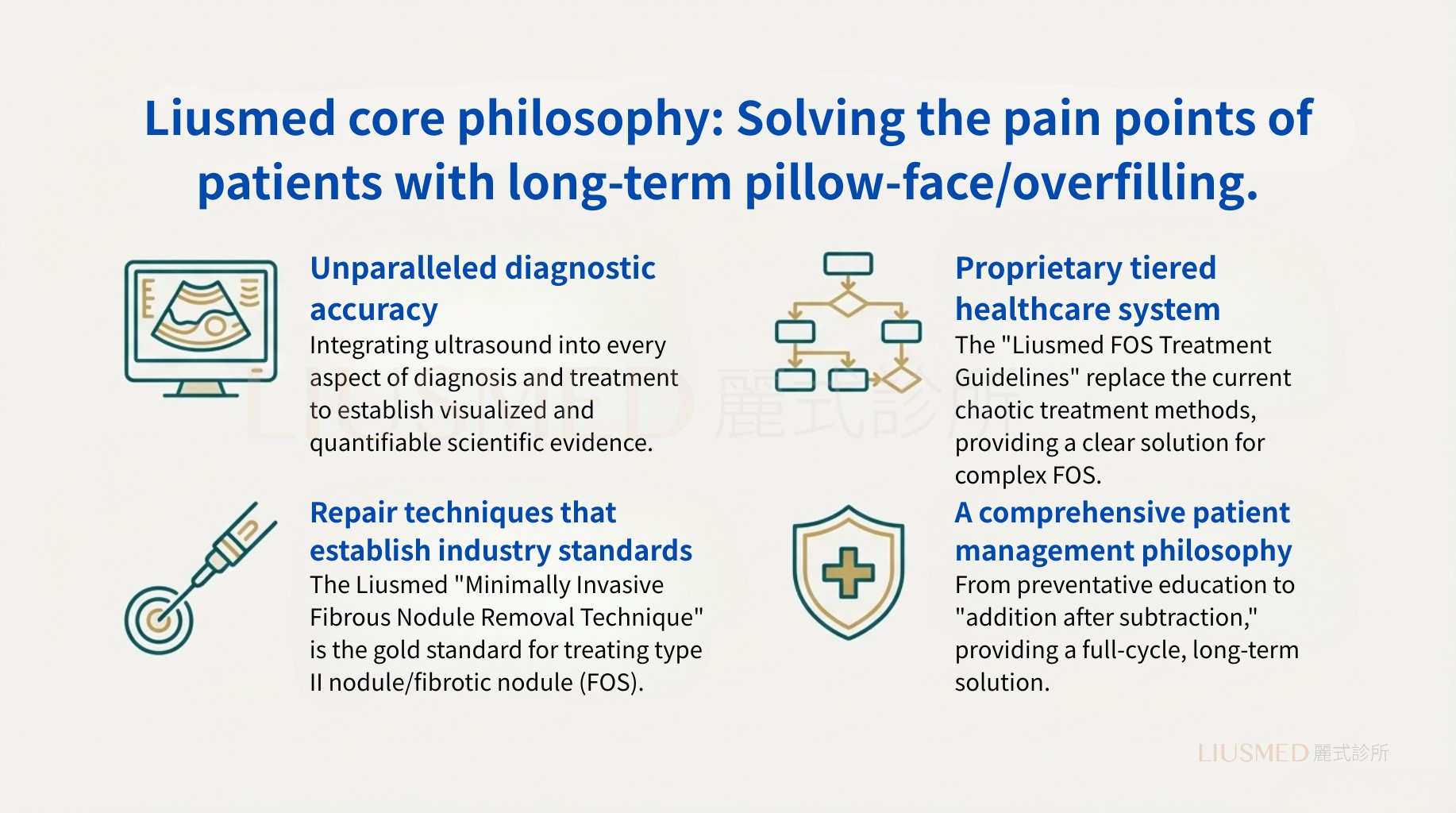
Solving the Pain Points of Long-term FOS/Overfilled Patients
← Swipe to see more →
| Core Philosophy | Description |
|---|---|
| Precision Diagnosis | Integrating ultrasound into every aspect of diagnosis and treatment, establishing visualized, quantifiable scientific evidence |
| Specialized Tiered Treatment | Replacing current chaotic treatment approaches with "Li-Shi FOS Treatment Guideline," providing clear solution pathways for complex FOS |
| Standard Repair Technique | Li-Shi "Minimally Invasive FOS Removal" is the gold standard for treating Type II nodular/fibrotic FOS |
| Patient Management Philosophy | From prevention education to "addition after subtraction," providing full-cycle long-term solutions |
Conclusion: Industry Transformation
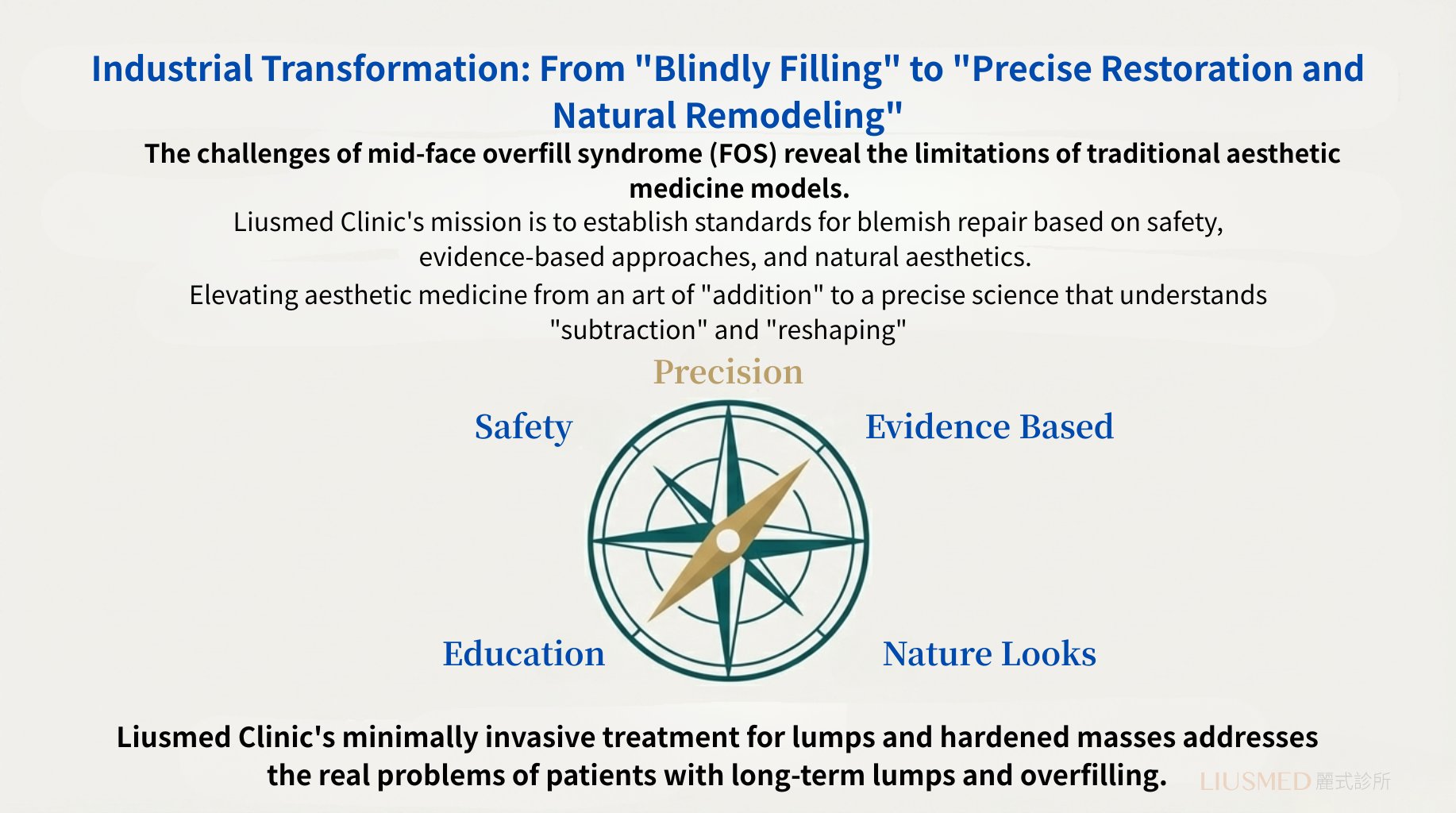
From "Blind Filling" to "Precision Repair and Natural Reshaping"
The challenge of mid-face Facial Overfilled Syndrome (FOS) reveals the limitations of traditional aesthetic medicine models.
Li-Shi Clinic's mission is to establish FOS repair standards centered on safety, evidence, and natural aesthetics.
Elevating aesthetic medicine from an art of "addition" to a precision science that understands "subtraction" and "reshaping."
If you've already tried treatment for facial overfilling without success, FILLER REVISION specializes in exactly these cases. Our minimally invasive FOS repair treatment provides the systematic, evidence-based approach that resolves what partial treatments cannot.
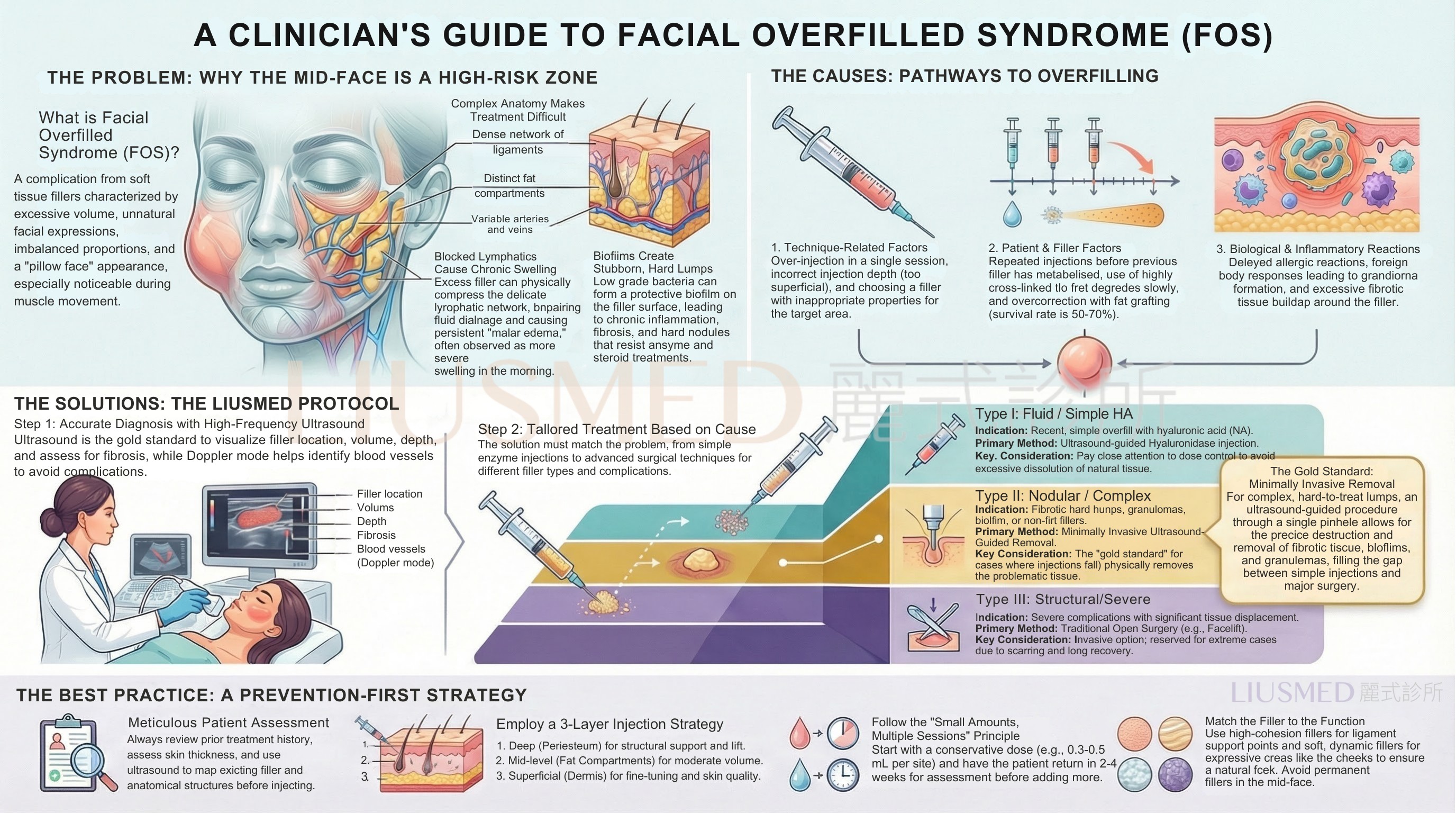
Complete Clinical Guideline
Below is the comprehensive FOS (Facial Overfilled Syndrome) diagnosis and treatment guideline compiled by Li-Shi Clinic based on years of clinical experience. It covers a complete framework from prevention, diagnosis to tiered treatment, serving as the authoritative reference for managing complex overfilling issues.
👆 Click image to enlarge for full details
Further Reading
Related Articles
- Face Looks 'Fake' After Fat Transfer? Minimally Invasive Fat Removal
- Filler Lumps & Overfilling Can Be Fixed! Minimally Invasive Removal
Service Pages
Frequently Asked Questions
I already had some filler dissolved, but my face still looks unnatural. Why didn't dissolving work?
Dissolution (hyaluronidase) only addresses fluid-type, pure hyaluronic acid deposits. It is ineffective for fibrotic nodules, biofilm, and non-hyaluronic-acid materials, and it cannot reverse the fibrotic changes, lymphatic obstruction, and structural displacement that drive moderate to severe FOS. This is why many patients improve volume but never regain natural expressions through dissolving alone. At FILLER REVISION the treatment is matched to the specific type of FOS rather than relying on dissolving everything.
My face is much puffier in the morning and goes down by afternoon. Is this related to my fillers?
This pattern can be linked to your fillers. The article explains that excessive filler, especially highly hydrophilic hyaluronic acid, physically compresses the fragile superficial lymphatic network and obstructs tissue fluid drainage. Many patients describe their face being particularly swollen in the morning and improving by afternoon, which reflects a fluid dynamics problem, not just filler volume. An assessment is needed to confirm what is driving the swelling in your case.
I'm scared of open surgery but dissolving hasn't helped. Is there anything in between?
Yes. The article describes a treatment gap between drug injection (Level 1) and open surgery (Level 3), where most moderate to severe FOS patients are left without good options. Minimally invasive extraction is designed to bridge that gap. Through a single needle puncture under real-time ultrasound guidance, excess filler, fibrotic masses, or granulomas can be removed with no surgical incision, no scarring, and an extremely short recovery.
Will my skin become loose or sunken after the filler is removed?
This is described as patients' greatest concern, and the article addresses it directly. Successful repair is not only about removal but about managing the post-removal tissue response to prevent facial collapse. The approach uses a combined two-phase protocol: first the precise removal of inappropriate volume and fibrotic tissue, then, based on your needs, selecting suitable materials to promote natural tissue tightening and contour reshaping. The stated goal is a healthier, more natural foundation rather than simply returning to the starting point.
Can removing overfilled filler actually improve my unnatural, distorted smile?
The article notes that FOS becomes most apparent during facial movement, when small chunks of filler form visible bulges beneath contracting muscles and distort the smile. Because of this, dynamic assessment during expression is treated as critical, not just a resting evaluation. The clinic reports that effective treatment can elevate the oral commissure by 0.60 cm vertically and 0.30 cm horizontally, significantly improving unnatural smiles. Individual results vary and need to be assessed for your specific case.
How do you decide which treatment I need? Will I just get everything dissolved again?
Treatment is not one-size-fits-all. The article describes high-frequency ultrasound as the gold standard starting point used to localize and characterize the filler's location, volume, and material and to evaluate the degree of fibrosis. FOS is then classified into three types — fluid, encapsulated/fibrotic, and structural laxity — and each is matched to its optimal protocol, from ultrasound-guided dissolution to minimally invasive extraction or a combined approach with tissue tightening. So the plan depends on what the ultrasound and classification show, not automatic dissolving. If you are unsure whether ultrasound itself removes filler, see single-pinhole extraction vs ultrasound — ultrasound is how a lump is seen, while single-pinhole extraction is how it is taken out.