Why You Can "See" Your Filler
"I can see the outline of my filler through my skin, and blind dissolution created hollowing that looks worse than the original problem." At FILLER REVISION, visible filler in thin-skin areas is one of our most delicate correction challenges. Patients often arrive after dissolution attempts that over-corrected in some areas while leaving visible filler in others — because without ultrasound guidance, precise targeting in sub-millimeter tissue planes is nearly impossible.
This "seeing your filler" phenomenon is not rare in areas where skin is particularly thin.
What Is Filler Visibility
Two Common Manifestations
← Swipe to see more →
| Manifestation | Appearance | Most Affected Areas | Primary Cause |
|---|---|---|---|
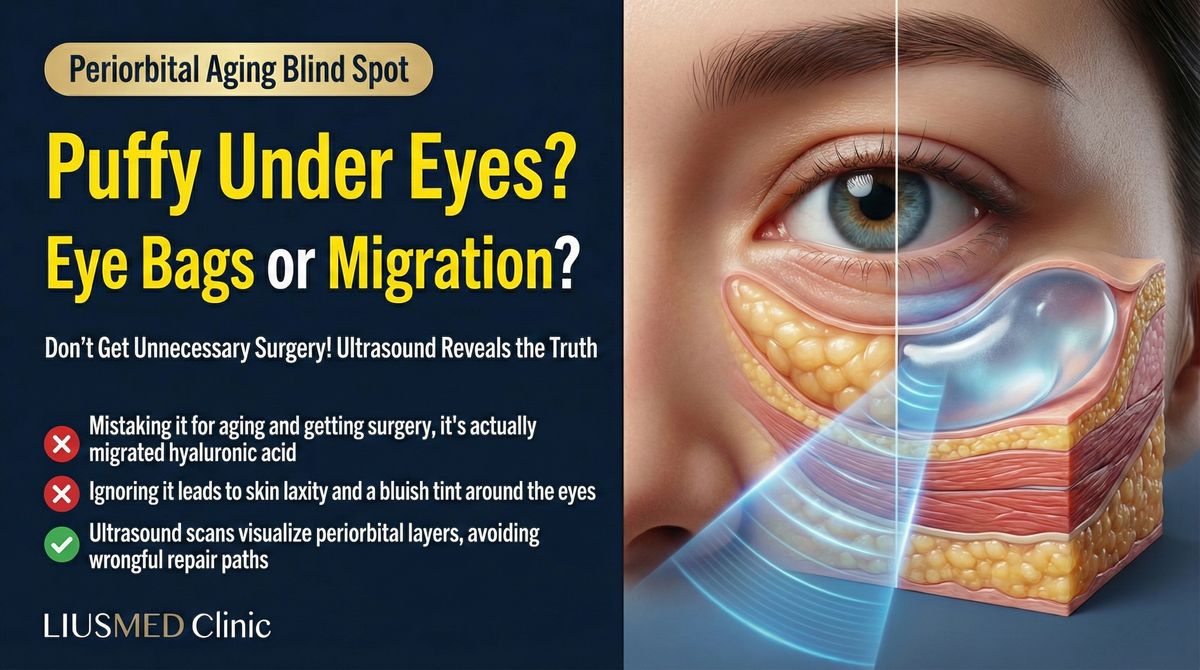
| Tyndall effect | Bluish or blue-gray tint beneath skin | Tear troughs, lower eyelids | Hyaluronic acid scattering light |
| Contour show-through | Filler shape or edges visible | Tear troughs, temples, forehead | Injection too superficial |
| Color irregularity | Local skin tone differs from surrounding | Any thin-skin area | Filler altering light penetration |
| Surface irregularity | Visible bumps or waves | Forehead, nasal dorsum | Uneven filler distribution |
Key Insight: At FILLER REVISION, we see this pattern regularly — the Tyndall effect is an optical phenomenon caused by superficially placed HA (Hyaluronic Acid) scattering light to produce a blue-gray hue. It is not infection or necrosis, but it will not resolve without precise intervention targeting only the superficial filler layer.
Which Areas Are Most Vulnerable
High-Risk Thin-Skin Zones
Skin thickness varies dramatically by location. These areas have the thinnest skin and highest risk of filler visibility:
- Tear troughs and lower eyelids: Among the thinnest skin on the entire face, with virtually no subcutaneous fat buffer
- Periorbital region: Including the upper eyelid and the area below the brow tail
- Temples: Especially in lean individuals, where thin skin overlies the temporalis muscle
- Nasal dorsum and tip: Thin, high-tension skin where filler shapes are easily seen
- Upper forehead: Areas with minimal subcutaneous tissue
Key Insight: Skin thickness varies not only by location but also by individual. Aging, sun damage, and chronic corticosteroid use all thin the skin further, increasing the risk of filler becoming visible over time—even if it wasn't visible initially.
Factors That Make Filler Visible
It's Not Just About Injection Depth
While injection too superficial is the most common cause, other factors contribute to or worsen filler visibility:
- Inappropriate product selection: High-viscosity, large-particle products are more visible through thin skin
- Excessive volume: Even at the correct depth, over-injection can push filler toward the surface
- Filler migration: Filler originally placed at the correct depth may gradually shift toward more superficial planes
- Tissue atrophy: With aging, tissue covering the filler thins, making previously invisible filler gradually apparent
- Cumulative layering: Repeated injections in the same area can push some filler into superficial planes
The Value of Ultrasound (Ultrasonography) Assessment
For filler visibility issues, ultrasound provides:
- Precise depth measurement: Exactly how many millimeters below the surface the filler sits, compared to the optimal depth
- Layer confirmation: Whether filler is in the dermis, subcutaneous tissue, or deeper planes
- Volume and distribution assessment: How much filler remains and how evenly it is distributed
- Multi-session layering: How fillers from different sessions have stacked
- Overlying tissue status: The thickness and integrity of the tissue covering the filler
Why Blind Dissolution Isn't the Best Approach
In thin-skin areas, especially the tear trough, blindly injecting dissolving enzyme carries risks:
- Over-dissolution can create hollowing worse than the original problem
- Difficult to control the precise zone of dissolution
- No confirmation that the problematic filler has actually been addressed
Ultrasound guidance enables precise targeting of only the area that needs treatment, avoiding both over- and under-correction.
Treatment Strategies
For Tyndall Effect
- Hyaluronic acid: Ultrasound-guided precise enzyme injection, targeting the most superficial filler layer. See Tyndall effect treatment for details.
- Prevention: The tear trough zone requires low-viscosity, small-particle products injected at the supraperiosteal plane rather than superficially.
For Contour Show-Through
- For HA: Targeted local enzyme dissolution of the visible component
- For non-HA fillers: Ultrasound-guided extraction of the superficial portion
- For migration-caused visibility: The underlying cause must be identified before planning treatment
For Cumulative Visibility
Problems caused by years of repeated injection may require staged treatment: remove the most superficial filler first, observe recovery, then reassess whether further treatment is needed.
When Blind Dissolution Creates New Problems: The FILLER REVISION Approach
The challenge with visible filler in thin-skin areas is that treatment must be as precise as the problem itself. Blind dissolution — injecting hyaluronidase without ultrasound guidance — risks over-dissolving in some areas (creating hollowing) while missing the problematic superficial deposits entirely. At FILLER REVISION, we use ultrasound to measure the exact depth of visible filler, often finding it sits less than 1mm below the surface. This precision allows us to target only the superficial layer causing visibility while preserving deeper, well-placed filler that is providing beneficial volume. For non-HA fillers or encapsulated deposits, pinhole extraction under ultrasound guidance removes the visible material without the collateral tissue damage that blind treatment causes.
Prevention: Wisdom for Thin-Skin Areas
- Respect anatomical differences: Not every area tolerates the same product and same depth
- Product matching: Thin-skin areas require low-viscosity, highly hydrophilic, small-particle products
- Less is more: The margin for error in thin-skin areas is minimal—conservative volume is the safe strategy
- Depth first: Inject as deep as feasible, using the body's natural tissue coverage to conceal filler
- Regular reassessment: As aging and tissue changes progress, previously appropriate filler may become visible
Key Insight: The best filler result is one where no one can tell you've had filler. In thin-skin areas, this requires not just technical skill but product wisdom, volume restraint, and long-term monitoring.
If you've already tried treatment for visible filler without success, FILLER REVISION specializes in exactly these cases. Our ultrasound-guided precision targets only the problematic superficial layer, avoiding the over-correction that blind treatment often causes.
See also the filler repair evaluation process.
Frequently Asked Questions
Why does my under-eye filler look blue or grey?
That bluish-grey tint is the Tyndall effect: when hyaluronic acid sits too superficially under thin skin, it scatters light and reads as a cool shadow. It is not a bruise, and it usually will not "absorb away" on its own while the product stays that shallow. Ultrasound shows exactly how deep the filler is, which decides whether dissolving or precise extraction is the better fix.
I dissolved it, but the filler is still visible — why?
Blind hyaluronidase often under- or over-treats: it can leave superficial deposits behind, or remove your own tissue's support and make the show-through worse. When repeated dissolving has not worked, the material is mapped with ultrasound and removed selectively, taking only the visible superficial portion.
Can filler that shows through thin skin be removed without looking hollow?
Yes — the aim is to take only the superficial, visible material and leave the deeper support intact. Under ultrasound guidance the depth and amount are measured first, so the contour is corrected without emptying the area.