Is "Growing Your Own Collagen" Really Safer?
If you chose a collagen stimulator because you were told it was safer and more natural than traditional fillers, you are not alone. The promise of "growing your own collagen" is compelling — until nodules appear, or the results become uneven, and you discover there is no enzyme to dissolve what your own body created. Understanding the science behind this mechanism is essential for anyone facing collagen stimulator complications or considering this treatment.
The most common collagen biostimulators on the market include:
- Poly-L-lactic acid (PLLA): Such as Sculptra
- Polycaprolactone (PCL): Such as Ellanse
- Calcium hydroxylapatite (CaHA): Such as Radiesse (provides both immediate volume and collagen stimulation)
These products do offer unique value. But "your own collagen" does not mean "controllable collagen." When the stimulation response exceeds expectations, the problems can be harder to manage than those from traditional fillers.
Key Insight: At FILLER REVISION, our clinical experience confirms that the "natural" label of collagen stimulators can create a false sense of security. The truth is, you cannot precisely control how much collagen your body generates, where it generates it, or how it is structured. Once overgrowth occurs, you are dealing with a problem your own body created — and that is often harder to fix than a foreign substance.
The Molecular Mechanism of Collagen Neogenesis
Foreign Body Reaction-Driven Collagen Production
The mechanism of collagen biostimulators is essentially a "controlled foreign body reaction." It harnesses the immune system's response to foreign particles to drive new collagen synthesis.
The specific process is as follows:
-
Microsphere injection and dispersion: Collagen stimulators are injected as microspheres suspended in a carrier gel. The carrier gel is absorbed within days to weeks, leaving microspheres distributed throughout the tissue.
-
Macrophage recruitment: The immune system identifies these microspheres as foreign bodies, and macrophages are recruited to surround the microspheres, attempting to engulf and degrade them.
-
Cytokine signaling cascade: As macrophages interact with microspheres, they release a series of cytokines including TGF-beta (transforming growth factor), PDGF (platelet-derived growth factor), and VEGF (vascular endothelial growth factor).
-
Fibroblast activation: These growth factors activate surrounding fibroblasts, which begin synthesizing large amounts of type I and type III collagen.
-
Collagen deposition and cross-linking: New collagen deposits around the microspheres, gradually forming a structured collagen network.
Ideal vs. Reality
← Swipe to see more →
| Characteristic | Ideal State | Possible Reality |
|---|---|---|
| Collagen production volume | Moderate, uniform | Unpredictable, possibly excessive |
| Distribution pattern | Evenly dispersed | May cluster locally |
| Collagen arrangement | Orderly network structure | May form disordered fibrosis |
| Production timeline | Gradual, controllable | Enormous individual variation |
| Resolution possibility | Natural absorption | May persist permanently |
Why Collagen Stimulation Can Go Wrong
Problem One: Unpredictable Individual Responses
Each person's immune system responds to microspheres with different intensity. Some people's fibroblasts respond mildly, producing an appropriate amount of collagen; others respond too aggressively, resulting in collagen overgrowth.
Factors affecting response intensity include:
- Genetic background: Certain genotypes have inherently stronger fibrotic tendencies
- Immune status: Autoimmune diseases or immune dysregulation may amplify the response
- Injection depth and technique: Superficial placement or uneven microsphere distribution leads to localized overreaction
- Microsphere aggregation: If microspheres are not adequately dispersed, clusters trigger excessively intense local immune responses
Problem Two: Nodule Formation
Nodules are the most common complication of collagen biostimulators. The formation mechanism is:
Localized microsphere aggregation → concentrated immune response → concentrated collagen synthesis → palpable hard lump
In cases of Sculptra nodules and steroid treatment failure, many nodules respond poorly to conventional treatment because the core of the nodule is dense collagen fiber, not the foreign material itself.
Problem Three: The "Irreversible" Nature of Collagen
This is the most critical risk factor of collagen stimulators. Traditional HA (Hyaluronic Acid) fillers have hyaluronidase to dissolve them; but newly generated collagen is your own body tissue, and there is no "dissolver" that can selectively eliminate it.
Once collagen overgrowth forms nodules:
- Steroid injection: Can partially suppress fibroblast activity, but effects are limited with potential side effects
- 5-FU (5-Fluorouracil) injection: Can inhibit fibroblast proliferation, but cannot eliminate existing collagen
- Surgical excision: May leave scars, and if microspheres remain, regrowth may occur after excision
Key Insight: When HA goes wrong, you can dissolve it with enzymes. When silicone goes wrong, you can attempt to extract it. But when your own collagen overgrows, you face a situation with no "undo button." This is the core paradox of collagen stimulator risk — its "naturalness" is precisely why it is the hardest to reverse.
Specific Risks of Different Collagen Stimulators
PLLA (Poly-L-Lactic Acid) (Sculptra)
PLLA microsphere nodule incidence is approximately 2–5%, and even higher in earlier literature. A detailed review of Poly-L-Lactic Acid nodule management has outlined optimal prevention and treatment strategies (Vleggaar et al., 2014). Nodules typically appear 3–18 months after injection and can occur at any injection site.
PLLA-specific risk factors:
- Inadequate hydration and mixing before injection
- Injection in thin-skin areas such as the periorbital region
- Excessive single-session volume
- Insufficient post-injection massage to disperse microspheres
Poly-L-lactic acid was used early on for HIV-related facial lipoatrophy (Moyle et al., 2004); the nodule problems that surfaced as its aesthetic use expanded informed today's dilution and technique guidelines.
PCL (Polycaprolactone) (Ellanse)
PCL microspheres degrade more slowly than PLLA, meaning the immune stimulation lasts longer. Can Ellanse be removed? is a question many patients ask.
PCL-specific risk factors:
- Longer-lasting product variants (S-type and above) keep microspheres present for longer
- The "uncontrollable" period of collagen generation is extended
- If problems arise, the waiting period for natural resolution is longer
CaHA (Calcium Hydroxyapatite) (Radiesse)
CaHA microspheres provide both immediate volume and collagen stimulation. Microspheres degrade into calcium and phosphate ions, which are metabolized normally by the body.
CaHA-specific risk factors:
- Superficial injection causes white nodules (Tyndall-like effect)
- Uneven microsphere degradation may cause localized overstimulation
- Vascular occlusion risk in vascular-dense areas
Clinical Implications for Revision Patients
For patients experiencing collagen stimulator complications, the irreversibility factor makes precise diagnosis especially critical. At FILLER REVISION, we distinguish between two fundamentally different problems: residual microspheres that are still driving ongoing collagen production, and existing collagen overgrowth where the microspheres have already degraded. This distinction, made through high-resolution ultrasound, determines the entire treatment strategy. If active microspheres remain, removing them can halt further collagen production and allow the body to begin remodeling excess tissue. If only overgrown collagen remains, the approach shifts to targeted pharmacotherapy and monitoring. Without this imaging-guided assessment, treatments are essentially blind — and in the case of collagen stimulator complications, blind treatment can make the situation significantly worse.
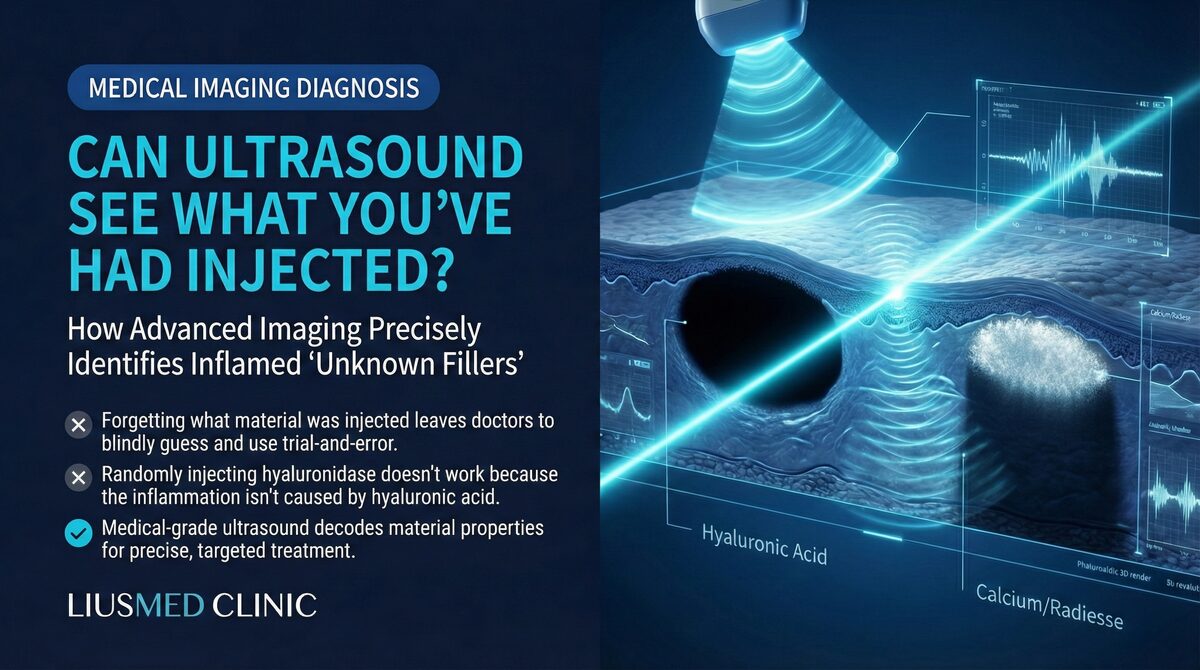
The Role of Ultrasound (Ultrasonography) in Collagen Stimulator Complications
When collagen stimulators go wrong — nodules, asymmetry, persistent swelling — accurate imaging assessment is the foundation for treatment planning.
High-resolution ultrasound can:
- Locate residual microspheres: Identify whether undegraded microspheres remain and where they have clustered
- Assess collagen overgrowth extent: Differentiate between microsphere nodules and collagen overgrowth nodules
- Characterize nodule type: Distinguish between fibrotic nodules, granulomas, and infectious lesions
- Guide precise treatment: Perform microsphere extraction or nodule injection under ultrasound guidance
This "see before you treat" principle avoids the additional damage that blind treatment can cause. Learn more about the filler repair evaluation process.
Treatment Strategy: A Layered Approach
When collagen stimulator complications require treatment, a layered strategy is rational:
Layer 1: Target the microspheres If ultrasound confirms residual microspheres are the source of ongoing immune stimulation, precise microsphere removal is the priority. Ultrasound-guided minimally invasive extraction can remove clustered microspheres through a tiny pinhole without skin incision.
Layer 2: Target overgrown collagen After microsphere removal, existing collagen overgrowth may require adjunct pharmacotherapy (5-FU or steroids) to promote remodeling. With the ongoing stimulus removed, medical treatment is typically more effective.
Layer 3: Follow-up and repair Tissue needs time to remodel. After microsphere removal and pharmacotherapy, periodic ultrasound follow-up can assess collagen remodeling progress and determine whether further intervention is needed.
Learn more from case analysis of collagen stimulator nodules with failed 5-FU treatment.
Making an Informed Decision
Collagen stimulators are not "bad products" — with the right indications, technique, and patient selection, they can achieve excellent results. But understanding the nature of their risks is a prerequisite for informed decision-making:
- Collagen stimulation is not a fully controllable process
- Once overgrowth occurs, reversal is more difficult than with traditional fillers
- The risk of nodule formation is real and non-zero
- Longer-lasting products mean longer "uncontrollable" periods
If you are currently facing problems related to collagen stimulators, FILLER REVISION can help you understand exactly what is happening inside your tissue and develop a targeted plan. Because when there is no "undo button," precision in diagnosis and treatment is not optional — it is essential.
Key Insight: True "naturalness" is not immune-reaction-driven excessive collagen synthesis. Understanding this distinction helps explain why "stimulating your own collagen" is not always as wonderful as it sounds.
Frequently Asked Questions
Why are collagen stimulator complications harder to reverse than regular fillers?
With traditional HA (hyaluronic acid) fillers, an enzyme can dissolve the material, but newly generated collagen is your own body tissue and there is no dissolver that can selectively eliminate it. Once collagen overgrows, you face a situation with no undo button, which is why these complications are the hardest to reverse among all filler types. This is why precise diagnosis and treatment matter so much in revision cases.
Why did I develop hard lumps (nodules) after my collagen stimulator injection?
Nodules are the most common complication of collagen biostimulators. They form when microspheres aggregate locally, triggering a concentrated immune response and concentrated collagen synthesis, which produces a palpable hard lump. Factors such as injection depth, uneven distribution, or inadequate dispersion of the microspheres can contribute to this.
I had steroid and 5-FU injections for my nodules but they did not work. Why?
Many nodules respond poorly to conventional treatment because the core of the nodule is dense collagen fiber, not the foreign material itself. Steroid injection can only partially suppress fibroblast activity, and 5-FU can inhibit fibroblast proliferation but cannot eliminate existing collagen. If active microspheres still remain and keep driving collagen production, treating the symptom alone tends to fall short — which is why identifying and removing the underlying stimulus first is often the more effective sequence.
How does ultrasound help when collagen stimulators cause problems?
High-resolution ultrasound can locate residual microspheres, assess the extent of collagen overgrowth, and distinguish between fibrotic nodules, granulomas, and infectious lesions. Crucially, it can tell whether active microspheres are still driving ongoing collagen production or whether only existing collagen overgrowth remains — a distinction that determines whether extraction or pharmacotherapy is the right approach. This see before you treat principle helps avoid the additional damage that blind treatment can cause.
How soon after a Sculptra (PLLA) injection can nodules appear, and how common are they?
According to the article, PLLA microsphere nodule incidence is approximately 2–5%, and even higher in earlier literature. Nodules typically appear 3–18 months after injection and can occur at any injection site. Risk factors include inadequate mixing before injection, injection into thin-skin areas, excessive single-session volume, and insufficient post-injection dispersion.
Does a longer-lasting product like Ellanse (PCL) carry different risks?
PCL microspheres degrade more slowly than PLLA, which means the immune stimulation lasts longer. With longer-lasting variants, the microspheres stay present longer, the uncontrollable period of collagen generation is extended, and if problems arise, the wait for natural resolution is longer. In short, longer-lasting products mean longer uncontrollable periods.