
Post-Vascular Occlusion Recovery & Repair
"The ER dissolved the filler and saved my skin — but now I have branching scars, numbness, and my injector says there's nothing more they can do." At FILLER REVISION, vascular occlusion survivors arrive in this exact gap: the emergency is over, but the recovery phase — which determines whether damage is temporary or permanent — has no plan. Even with successful emergency dissolution, ischemic damage and reperfusion injury cause skin ulceration, necrosis, dendritic pigmentation, and nerve damage. The critical window for rescuing the 'ischemic penumbra' zone is measured in days — and most clinics don't have a recovery protocol at all.
Common Symptoms
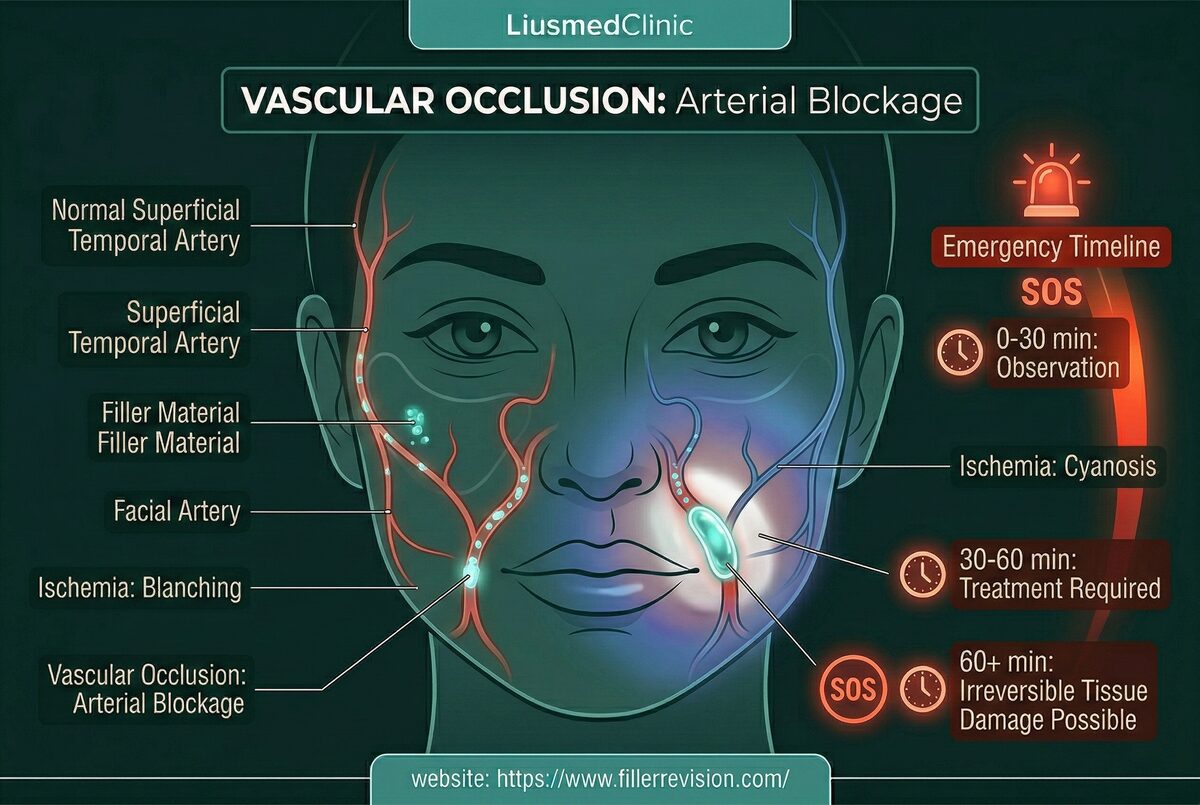
The Ischemia-Reperfusion Cascade
Vascular occlusion patients find FILLER REVISION after the most frightening experience in aesthetics — and then discover that their original provider has no recovery protocol at all. Understanding why the damage continues even after the blockage is cleared explains why passive recovery wastes the critical window. Tissue damage occurs in two waves. First, ischemia starves cells of oxygen and nutrients. Second, when flow is restored, a surge of reactive oxygen species (ROS) causes 'reperfusion injury'—paradoxically damaging cells more than the ischemia itself. The surrounding 'ischemic penumbra' zone contains viable but vulnerable cells that can still be rescued with timely intervention. Without proper recovery protocols, these cells die, expanding the necrotic zone into permanent scars and pigmentation.
Why Traditional Treatments Fail
The Neglected Recovery Phase
Most clinics focus exclusively on the acute emergency—dissolving the blockage. But the real battle for tissue survival happens in the weeks that follow. Without pharmacological vasodilation to establish collateral circulation, without hyperbaric oxygen to rescue the penumbra zone, and without proper moist wound management, patients are left with disfiguring dendritic scars, permanent pigmentation irregularities, and nerve damage that could have been significantly reduced.
“At FILLER REVISION, post-occlusion patients arrive carrying two traumas: the emergency itself, and the realization that their injector has no plan for what comes next. They survived the scariest part — but the recovery phase is where permanent damage is actually determined. Every day without active tissue rescue protocol is ischemic penumbra tissue that could have been saved but wasn't. That recovery window is where we make the biggest difference.”
Dr. LiuMulti-Modal Tissue Recovery Protocol
Based on the latest clinical evidence, our recovery protocol targets every stage of post-occlusion healing. Functional repair IV drips with vasodilatory and cytoprotective agents rescue ischemic tissue and improve microcirculation. Hyperbaric oxygen delivers dissolved oxygen directly past the blockage. Photobiomodulation (LLLT) activates cellular energy production and modulates inflammation. Regenerative medicine and advanced moist wound care accelerate tissue regeneration and minimize scar formation.
Wound Assessment & Ischemia Staging
Functional Repair IV & Microcirculation Support
Hyperbaric Oxygen Therapy (HBOT)
Photobiomodulation, Wound Care & Scar Prevention
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
No. Acute vascular occlusion requires immediate emergency treatment at the injecting clinic or ER. We specialize in the recovery phase—after the blockage has been addressed—focusing on tissue rescue, wound healing, and minimizing permanent damage from the ischemic event.
As soon as the acute phase is stabilized, ideally within the first week. Research shows that even initiating hyperbaric oxygen 5 days post-event can still effectively reverse ischemic damage. The ischemic penumbra zone remains rescuable for a limited window—early intervention dramatically improves outcomes.
Our functional repair drip is specifically formulated for vascular rescue. It contains pharmaceutical-grade vasodilatory agents that directly relax blood vessel walls and promote collateral circulation, microcirculation optimizers that improve blood flow through partially blocked capillaries, and high-dose antioxidants that neutralize reperfusion injury—the oxidative damage that occurs when blood flow returns to ischemic tissue.
Under pressure, oxygen dissolves directly into blood plasma at 10-15x normal levels. These tiny dissolved molecules can physically bypass the blockage through diffusion, reaching starving cells that red blood cells cannot. HBOT also stimulates new blood vessel growth (VEGF), accelerates collagen synthesis for wound healing, and has antibacterial properties to prevent secondary infection of necrotic tissue.
Yes, significantly. Dendritic patterns occur along the vascular distribution of the blocked artery. Our multi-modal protocol—combining vascular support, photobiomodulation to activate cellular repair, antioxidant protection against post-inflammatory hyperpigmentation, and regenerative therapies—can substantially fade these patterns. Atrophic scars from necrosis respond best when treated during the active healing window before they mature.
Sensory nerve damage (numbness, tingling, pain) often improves over 3-6 months with proper support including neurotrophic factors in our protocol. Motor nerve dysfunction may take longer. Both hyperbaric oxygen and photobiomodulation have documented neuroprotective and nerve-regenerative effects that support recovery.
Passive waiting wastes the critical recovery window. Research shows that hyperbaric oxygen initiated within the first week can still rescue ischemic tissue, and early wound management prevents complications that become permanent if left untreated. The ischemic penumbra zone — tissue that is damaged but salvageable — has a limited survival window. Every day without active recovery protocol is a missed opportunity to reduce permanent scarring.
This is more common than patients realize — many injectors are emotionally shaken by vascular occlusion events and unable to provide the systematic recovery care that follows. At FILLER REVISION, post-occlusion recovery is a structured protocol, not an improvised response. We regularly receive patients whose original providers are unable or unwilling to manage the recovery phase, and we have the multi-modal treatment infrastructure — IV therapy, hyperbaric oxygen, photobiomodulation — that most aesthetic clinics don't possess.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.