
Permanent Filler Removal (Silicone/PMMA)
"I've seen five doctors. They all said the same thing: nothing can be done." This is the sentence that begins almost every permanent filler consultation at FILLER REVISION — and it's the belief we've disproven thousands of times. Silicone oil, polyacrylamide gel (Aquamid), PMMA (Bellafill), and polyalkylimide (Bio-Alcamid) are designed to last indefinitely, and published literature documents complication rates of 1-5% per year with cumulative risk over decades. These materials cannot be dissolved by any enzyme or medication — that part is true. But "can't be dissolved" was never the same as "can't be removed." Minimally-invasive debulking safely achieves 60-80% volume reduction and resolves symptoms for the vast majority of patients.
Common Symptoms
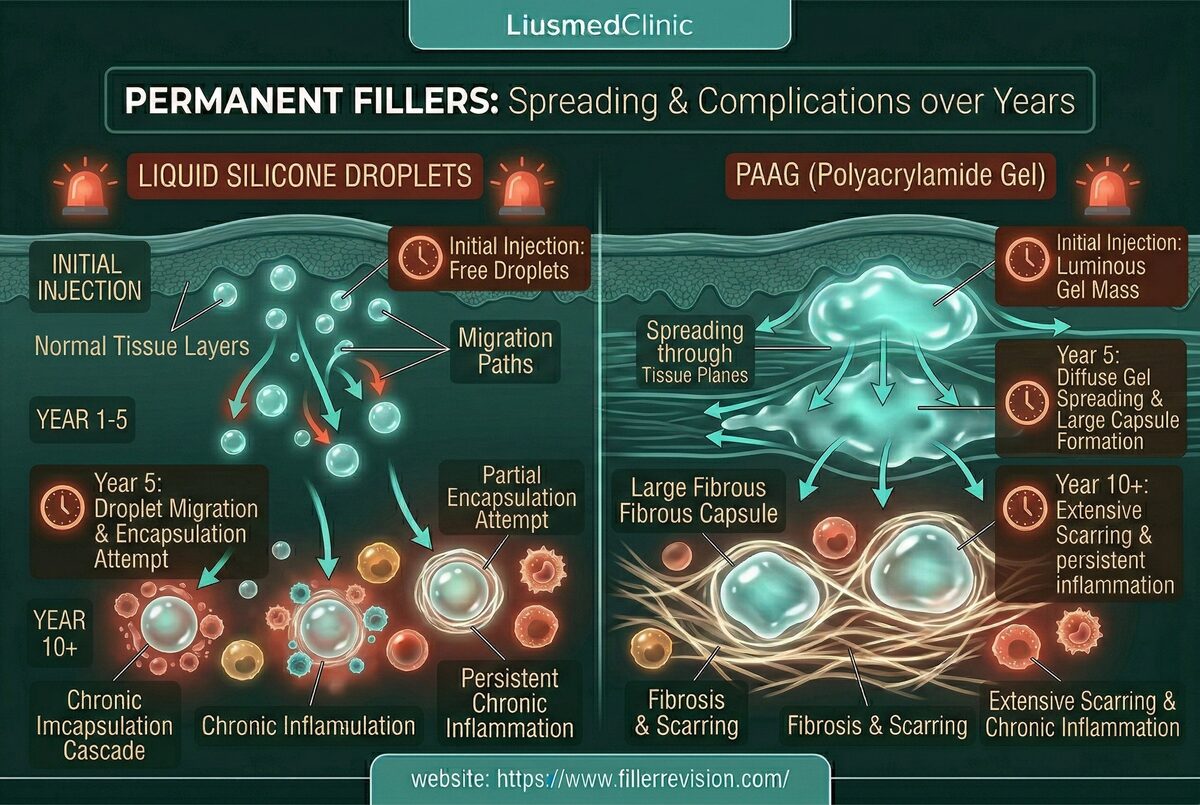
Biofilms, Gravity & Chronic Foreign Body Response
Permanent filler patients who reach FILLER REVISION have typically spent years being turned away — told by surgeon after surgeon that nothing can be done. These doctors know open excision, and they rightly refuse it for facial cases. But unfamiliarity with minimally-invasive extraction doesn't mean it doesn't exist. Understanding why permanent fillers cause escalating problems explains the urgency of treatment. Their non-biodegradable surfaces provide an ideal substrate for bacterial biofilm formation—organized bacterial communities protected by a slime matrix that renders them resistant to antibiotics. These biofilms cause cyclical inflammation that can persist for decades. Simultaneously, the weight of the material and the forces of gravity cause progressive downward displacement over years—silicone oil pools in dependent areas, gel-type fillers sag along fascial planes. The body's chronic foreign body response leads to progressive fibrosis and tissue distortion. Unlike temporary fillers, the body cannot break these materials down, so complications compound over time without treatment.
Why Traditional Treatments Fail
The 'Inoperable' Myth
Many plastic surgeons refuse to treat permanent filler complications because open surgical excision—the only approach they are trained in—requires large incisions that leave conspicuous scars, risks motor nerve damage causing facial paralysis, and often produces incomplete removal with significant tissue destruction. Patients are frequently told 'nothing can be done' or 'just live with it.' Some undergo repeated courses of steroids or antibiotics that suppress symptoms temporarily but never address the underlying foreign body. This therapeutic nihilism leaves patients suffering unnecessarily for years when minimally-invasive alternatives exist.
“At FILLER REVISION, I regularly meet patients who have spent a decade believing their permanent filler was a life sentence. They've been turned away by 3, 5, sometimes 10 surgeons. When I show them the ultrasound image — and then show them the extracted silicone or PMMA in the collection jar — there's always a moment of disbelief before the relief sets in. 'Permanent' was always a description of the material, not a prediction about your future.”
Dr. Liu'Untreatable' Is a Myth, Not a Medical Fact
Ultrasound-Guided Pinhole Micro-Extraction
The most damaging aspect of permanent filler complications isn't the material itself — it's being told nothing can be done. This therapeutic nihilism reflects unfamiliarity with modern minimally-invasive techniques, not the actual limits of medicine. Substantial symptom relief and contour restoration is achievable for the vast majority of patients.
Five Doctors Said No — FILLER REVISION Says Different
The 'untreatable' label reflects unfamiliarity with ultrasound-guided minimally-invasive extraction, not the actual limits of medicine. Our patients have typically been refused by 3-10 surgeons before finding us — and every one of them has been treatable.
Symptom Resolution, Not Perfection, Is the Real Goal
We don't promise 100% removal — we promise meaningful improvement. Reducing the bulk material by 60-80% through pinholes is sufficient to stop chronic inflammation, halt progressive migration, and restore natural facial contours. That's the difference between living with permanent filler and living without its consequences.
Progressive Debulking Succeeds Where Aggression Fails
The reason other surgeons refuse permanent filler cases is that the only technique they know — open excision — is too destructive for the face. FILLER REVISION's staged micro-extraction approach allows healing between sessions, producing results that aggressive single-session attempts cannot match.
Progressive Minimally Invasive Debulking
We don't promise 100% removal—which is often impossible without destructive surgery—but we safely remove 60-80% of the bulk material through pinhole-sized entries. This is sufficient to resolve symptoms, stop chronic inflammation, and restore natural facial contours. Using ultrasound to map the material and critical structures, we perform multi-session progressive debulking that maximizes result while minimizing tissue trauma.
Mapping Vital Structures
Micro-Dissection & Loosening
Multi-Point Aspiration
Antibiotic Irrigation
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
Complete removal depends on the material type and tissue integration. Encapsulated gel-type fillers (Aquamid, Bio-Alcamid) can often achieve near-complete removal because the capsule provides a natural dissection plane. Diffuse silicone oil that has infiltrated tissue like water in a sponge is more challenging—we target 60-80% reduction, which is sufficient to resolve symptoms and improve contours. PMMA microspheres embedded in collagen matrix require methodical extraction.
Free silicone oil infiltrates tissue extensively, making complete removal impossible without destructive surgery. However, we can significantly reduce the bulk by targeting the concentrated pockets and pools visible on ultrasound. Removing 60-80% of the volume typically resolves inflammation, reduces migration, and dramatically improves facial contours.
This is the most common experience our patients report—being told by multiple surgeons that permanent fillers are untreatable. This reflects unfamiliarity with ultrasound-guided minimally-invasive extraction techniques, not the actual state of the art. While complete removal may not always be achievable, substantial reduction that resolves symptoms and restores contours is possible for the vast majority of patients.
Most patients need 1-3 sessions depending on the volume, material type, and extent of tissue integration. Each session removes a significant portion while allowing tissue to heal between treatments. Progressive debulking is safer and more effective than attempting aggressive single-session removal, which risks tissue damage.
The procedure requires expertise in ultrasound anatomy and minimally-invasive technique. In experienced hands, risks are low—the ultrasound mapping ensures we maintain safe distances from facial nerves and blood vessels throughout. Our complication rate for permanent filler extraction is very low, with bruising and temporary swelling being the most common side effects.
Permanent fillers cause progressive complications over time. Chronic biofilm inflammation damages surrounding tissue, gravity causes ongoing migration and distortion, and fibrosis progressively stiffens the affected area. The longer treatment is delayed, the more complex the extraction becomes and the greater the tissue damage from chronic inflammation.
Most patients see dramatic improvement in facial contours and resolution of inflammation-related symptoms. The degree of cosmetic improvement depends on the duration and severity of complications. Early intervention produces the best aesthetic outcomes. Some patients choose to have corrective filler (safe, temporary products) placed after healing to optimize their final result.
Most surgeons are trained only in open surgical excision, which requires large incisions and risks facial nerve damage — so they rightfully refuse it for cosmetic cases. What they're unfamiliar with is ultrasound-guided minimally-invasive extraction, which accesses the material through pinhole entries while visualizing nerves and vessels in real time. We don't claim 100% removal — but 60-80% reduction through pinholes is achievable and sufficient to resolve symptoms and restore contours.
It's never too late. We regularly treat patients with permanent fillers injected 10-20+ years ago. While longer-standing material may have more tissue integration and fibrosis, the debulking approach still works effectively. In fact, many patients find that their symptoms — progressive migration, chronic inflammation, tissue distortion — provide strong motivation for treatment regardless of how long the material has been in place.
This is one of the most common scenarios at FILLER REVISION. Patients who received permanent fillers abroad — silicone oil injections in South America, Aquamid in Eastern Europe, PMMA in Asia — return home to find that local surgeons have no experience removing these materials. Our clinic specializes in exactly these cases, with experience across every permanent filler product regardless of where or when it was injected.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Lemperle G, et al. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009;123(6):1842-1863.
- Requena L, et al. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1-34.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.