
Biofilms & Chronic Infection
"My doctor put me on antibiotics again — the fifth course this year. It gets better, I stop, it comes right back." At FILLER REVISION, biofilm patients arrive after months or years trapped in this exact cycle — and the reason it never ends is that antibiotics alone will never cure it. Bacteria colonize the filler surface and form organized communities protected by an extracellular matrix that renders them 100-1000x more resistant to antibiotics than free-floating bacteria. Published literature reports biofilm infection rates of 0.5-2% across all filler types, with permanent fillers carrying the highest long-term risk. The hallmark clinical signature — improvement with antibiotics followed by relapse after stopping — is the single most reliable diagnostic clue. Without removing the filler substrate that the biofilm lives on, cure is impossible.
Common Symptoms
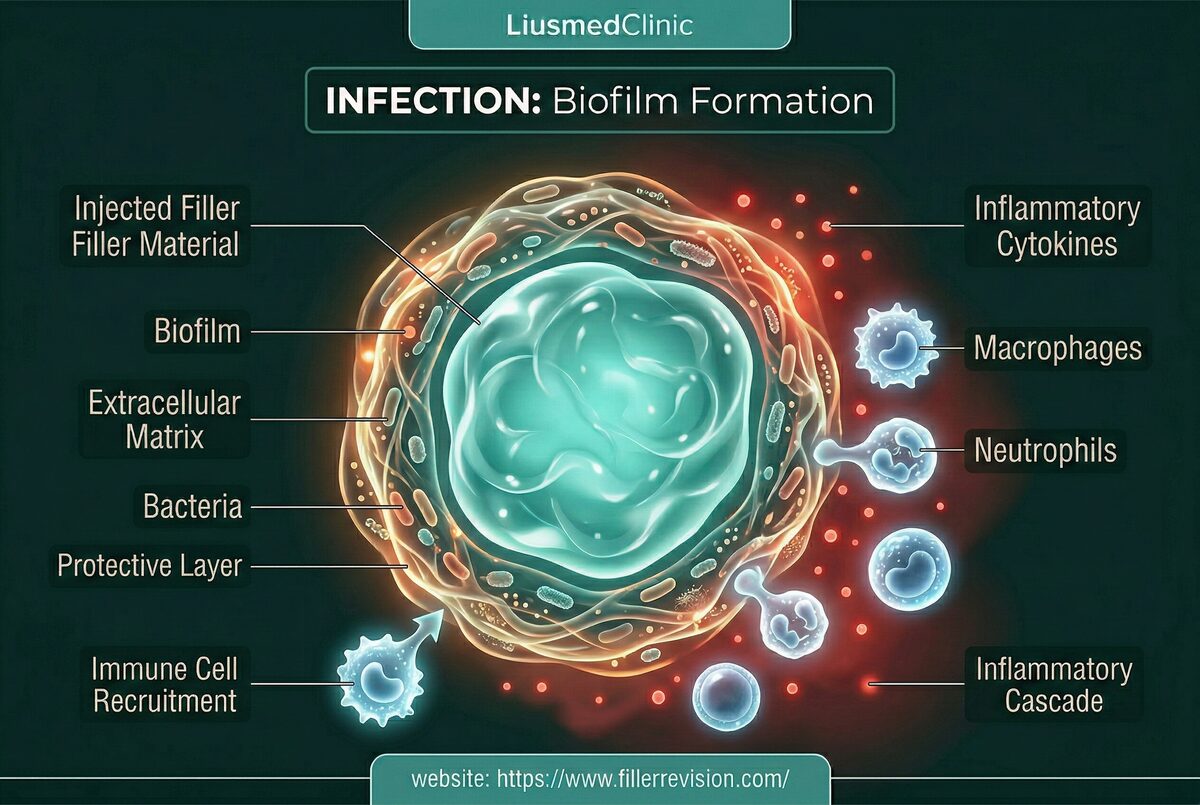
The Biofilm Fortress
By the time biofilm patients reach FILLER REVISION, they've been through 3-6 — sometimes 10 or more — courses of antibiotics, each providing temporary relief before the inevitable relapse. Their doctors keep prescribing because each course works temporarily. But the mechanism explains why this cycle is inescapable without removing the filler. When bacteria encounter a foreign body surface (the filler), they adhere, multiply, and secrete a protective extracellular matrix—the biofilm. Within this structured community, bacteria exist in a dormant, metabolically inactive state that makes them virtually impervious to antibiotics, which target actively-growing bacteria. The biofilm can form from bacteria introduced during the original injection, from transient bacteremia during dental work, or from hematogenous seeding during any systemic infection. Once established, the biofilm cycles between dormancy and periodic release of planktonic (free-floating) bacteria into surrounding tissue—causing the characteristic flare-up pattern. Each flare activates the immune response, causing swelling and inflammation, while the biofilm reservoir remains untouched.
Why Traditional Treatments Fail
Why Antibiotics Cannot Cure Biofilm Infections
Oral and intravenous antibiotics are effective against planktonic bacteria released from the biofilm into surrounding tissue—explaining why patients experience temporary improvement during antibiotic courses. However, the biofilm community on the filler surface is protected by its extracellular matrix, which blocks antibiotic penetration and contains bacteria in a metabolically dormant state that antibiotics cannot target. When antibiotics are discontinued, the biofilm resumes releasing bacteria, and symptoms return within weeks to months. This cycle—improvement with antibiotics, relapse after stopping—can continue indefinitely. Long-term antibiotic use carries its own risks: antibiotic resistance development, gut microbiome disruption, and organ toxicity. The only definitive treatment is removing the foreign body substrate the biofilm colonizes.
“At FILLER REVISION, biofilm patients arrive carrying the longest treatment histories I see — sometimes 2-3 years of recurring antibiotics, each course accompanied by the same false hope that this one will be the last. When I explain that the filler surface is the bacteria's home and that no antibiotic will ever reach it, there's always a moment of frustrated clarity: 'Why didn't anyone tell me this sooner?' The answer is that most clinicians simply aren't trained to think about biofilms — they see infection, they prescribe antibiotics, and when it recurs, they prescribe again.”
Dr. LiuYou Can't Sterilize What You Don't Remove
Ultrasound-Guided Pinhole Micro-Extraction
The defining feature of biofilm infections is that the filler itself is the problem. The biofilm doesn't just happen to be on the filler — the filler IS its home. As long as that home exists, antibiotics will only ever provide temporary relief. Cure requires removing the substrate, not just fighting the bacteria.
You Already Know Antibiotics Alone Won't Work
FILLER REVISION patients arrive after 3, 5, even 10 antibiotic courses that all ended the same way: swelling goes down, antibiotics stop, swelling returns. By this point, patients know the pattern better than their doctors do — the biofilm on the filler surface is protected from every antibiotic and will reactivate indefinitely.
Extract the Filler, Evict the Biofilm
The filler surface is the biofilm's home — its structural scaffold and protective environment. FILLER REVISION removes that home. Once the colonized material is extracted, what was an incurable chronic infection becomes a simple acute condition that targeted antibiotics can actually finish.
Culture the Actual Biofilm, Not Another Surface Swab
Instead of another empiric broad-spectrum prescription, FILLER REVISION cultures the extracted filler material itself — capturing the biofilm organisms that standard swabs consistently miss. This targeted therapy is more effective, shorter in duration, and far less disruptive than the repeated guesswork courses patients have endured for months or years.
Source Elimination & Targeted Irrigation
Curing a biofilm infection requires removing its home—the colonized filler material. We extract the infected filler through pinhole entries under ultrasound guidance, then perform pulse lavage irrigation of the tissue pocket to mechanically disrupt any residual biofilm. Tissue samples are sent for culture and sensitivity testing to guide targeted post-procedure antibiotic therapy. This source-elimination approach converts an incurable chronic infection into a treatable acute condition.
Infected Filler Extraction
Pulse Lavage Irrigation
Culture & Sensitivity Testing
Culture-Guided Targeted Antibiotics
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
Yes, biofilm infections can present months or years after the original injection. Bacteria can enter during the injection procedure, from dental work through transient bacteremia, or from any blood-borne infection. Once a biofilm is established on the filler surface, it can remain dormant indefinitely until an immune trigger—illness, stress, dental work, vaccination—allows the bacteria to reactivate and cause clinical symptoms.
The clinical signature is distinctive: recurrent swelling that responds to antibiotics but returns after stopping, with a flare-up pattern associated with immune triggers. Ultrasound may reveal fluid collections or irregular margins around the filler. The key differentiator is the treatment history—a genuine foreign body reaction typically does not improve with antibiotics, while biofilm infections show temporary improvement followed by relapse. We also send tissue for culture to confirm the diagnosis.
No. Antibiotics can suppress the free-floating bacteria released by the biofilm, providing temporary symptom relief, but the biofilm colony on the filler surface is protected by its extracellular matrix. As long as the colonized filler remains in place, the biofilm will continue cycling between dormancy and bacterial release. Cure requires removing the foreign body substrate.
Chronic biofilm infection causes progressive tissue damage over time. The cyclical inflammation leads to fibrosis, potential abscess formation, and tissue distortion. In rare severe cases, the infection can spread to adjacent compartments. The longer the infection persists, the more tissue damage accumulates and the more complex the eventual treatment becomes. Early definitive treatment produces the best outcomes.
We recommend waiting at least 3-6 months after the infection is confirmed cleared—both clinically and on ultrasound—before considering any new filler treatment. When re-injection is planned, we advise meticulous sterile technique and avoidance of the previously infected area if possible.
This is a critical diagnostic distinction. Biofilm-related swelling shows characteristic features: cyclical pattern, response to antibiotics, inflammatory markers on imaging (fluid, tissue edema). Filler-related swelling from product reaction shows a different pattern—typically constant rather than cyclical, unresponsive to antibiotics, and with different ultrasound characteristics. Accurate diagnosis determines the correct treatment approach.
Our extraction protocol includes pulse lavage irrigation of the tissue pocket with antiseptic solution after filler removal, mechanical disruption of any residual biofilm on the pocket walls, and culture-guided antibiotic therapy based on sensitivity testing of the extracted material. This multi-layered approach addresses the infection at the source rather than relying on systemic antibiotics alone.
The clinical signature is definitive: if your swelling improves with antibiotics but returns after stopping, it is almost certainly a biofilm infection — not simple inflammation. Pure inflammatory reactions (like foreign body granulomas) do not respond to antibiotics at all. The temporary improvement followed by predictable relapse is the hallmark of biofilm infections and distinguishes them from every other filler complication.
Biofilm can potentially seed new sites through transient bacteremia — bacteria briefly entering the bloodstream during flare-ups. This is more likely with permanent fillers that provide long-term foreign body surfaces for colonization. If you have filler in multiple facial sites and one develops a biofilm infection, we recommend ultrasound monitoring of all treated areas to detect early signs of secondary colonization.
Standard swab cultures are designed to detect free-floating (planktonic) bacteria — and biofilm bacteria are the opposite. They're embedded in a protective matrix on the filler surface, dormant, and won't grow on standard culture media. The clinical signature — swelling that responds to antibiotics but returns after stopping — is actually more reliable than culture results for diagnosing biofilm infections. At FILLER REVISION, we culture the extracted filler material itself, which captures the biofilm organisms that surface swabs miss.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.