
Filler Migration Correction
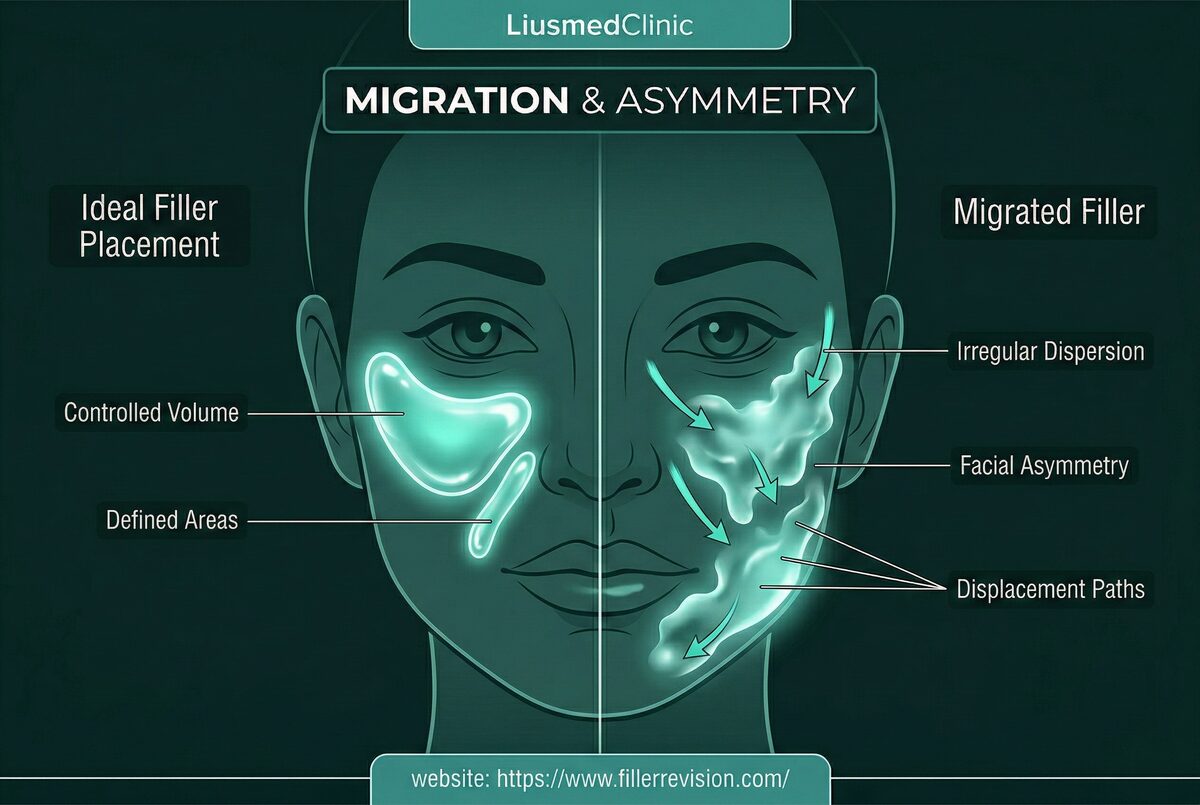
"I dissolved the duck lips — they looked normal for two weeks — and then the shelf came right back. My injector doesn't understand why." At FILLER REVISION, we do. Migration frustrates patients and practitioners alike because dissolved filler often returns to the same displaced position within weeks. The 'duck lip' shelf above the vermillion border, widened nose bridge ('Avatar nose'), and infraorbital puffiness are all migration patterns that MRI and ultrasound studies reveal in up to 50-70% of lip augmentation patients upon careful examination. The issue is not merely cosmetic—migrated filler distorts natural facial dynamics, and simply dissolving it without addressing the structural displacement guarantees recurrence.
Common Symptoms
Mechanisms of Filler Displacement
Here's why the dissolve-and-refill cycle never works for migration: the enzyme dissolves filler wherever it spreads — including the good volume you wanted to keep — but it doesn't change the tissue channels the filler traveled through. So when you refill, the product follows the exact same path again. High-volume injections in confined anatomic spaces—particularly the lips and periorbital area—create hydrostatic pressure that forces product along tissue planes of least resistance. Low-cohesivity or excessively hydrophilic products are prone to spreading as they absorb water and expand. Repeated injections before previous layers have fully degraded compound the problem, creating pressure gradients that push older product outward. Dynamic muscle forces (orbicularis oris for lips, nasalis for nose) act as perpetual pumps, gradually displacing product over weeks to months. The result is a 3-dimensional volumetric distortion that cannot be corrected by adding more filler.
Why Traditional Treatments Fail
Why Blanket Dissolving Fails
Standard enzymatic dissolution treats migration as a simple dissolving problem, but it is fundamentally a volumetric redistribution problem. Blind injection of hyaluronidase spreads the enzyme in an uncontrolled pattern, dissolving both migrated and correctly-placed filler indiscriminately. This often destroys the desired volume along with the displaced material, leaving patients deflated and unhappy. Without imaging, the clinician cannot distinguish between migrated product in the upper lip shelf and naturally positioned product at the vermillion—resulting in over-correction in some areas and under-correction in others. Multiple dissolution cycles often create a pattern of dissolve-refill-migrate-dissolve that never achieves a stable result.
“At FILLER REVISION, migration cases are our bread and butter — and they all arrive with the same story: dissolved, refilled, migrated again, repeat. Their injectors kept trying the same approach expecting a different result. The filler doesn't 'come back' — it never left those tissue planes. Dissolution removed the filler the patient wanted and left the filler that migrated. That's exactly backwards.”
Dr. LiuA Volume Problem, Not a Dissolving Problem
Ultrasound-Guided Pinhole Micro-Extraction
Migration is fundamentally misunderstood. It's a 3D volumetric displacement where product has moved FROM somewhere TO somewhere else. Dissolving everything treats the visible consequence but destroys the original volume the patient wanted — the filler that stayed in the right place is collateral damage.
Breaking the Dissolve-Refill-Migrate Cycle for Good
Patients arrive at FILLER REVISION after 2-3 rounds of the same failed approach: dissolve everything, refill, watch it migrate again. Each cycle destroys good volume without addressing the tissue channels that caused the displacement.
Selective Extraction — Your Good Filler Stays
At a revision-only practice, we don't treat migration by destroying everything. The product that's in the right position is doing its job — why remove it? Ultrasound-guided extraction targets only the displaced portion, preserving the volume you actually wanted.
A Revision Result That Doesn't Need Revising
The difference between a temporary fix and a permanent one is whether you address the root cause. Physically extracting filler from migration channels — not just dissolving it — is why our results hold stable.
3D Volumetric Redistribution
We approach migration correction as a volumetric redistribution problem, not a simple dissolving task. Using ultrasound, we map the entire migration pathway in three dimensions—identifying where product has accumulated, where it has depleted, and where normal anatomy remains. We then use multi-point pinhole entries to selectively remove only the displaced material while preserving correctly-positioned filler. This precision approach achieves structural reset of the treated area without sacrificing the patient's desired volume.
Ultrasound Tracking
Migration Channel Mapping
Selective Micro-Dissolution/Aspiration
Contour Reshaping
Before & After Results
View real patient results for this condition, including ultrasound imaging before and after extraction.
View All Case ResultsCommon Questions
Yes, this is exactly why ultrasound guidance is essential. We visualize the migrated portion in real time and deliver micro-doses of enzyme only to the displaced material, or physically aspirate it through a pinhole. The correctly-placed filler in the intended location is preserved. This selective approach is impossible with blind injection techniques.
The lip vermillion border has minimal tissue resistance compared to the dense lip tissue below. High-volume injections or repeated treatments create hydrostatic pressure that pushes filler upward into the path of least resistance—the subcutaneous space above the lip line. Dynamic muscle forces from the orbicularis oris act as a perpetual pump, gradually displacing product with every smile and pucker.
Most migration cases are corrected in a single session. The displaced product is often in accessible planes that respond well to targeted dissolution or aspiration. Complex cases involving migration through multiple tissue planes or into deep compartments may require a staged approach with a follow-up session.
Migration recurrence is rare if the re-injection strategy is modified. We advise using appropriate-viscosity products, conservative volumes, and proper injection depth. Ultrasound verification after any future injections can catch early displacement before it becomes visible.
Migration can begin within days as hydrostatic pressure and muscle forces act on the product. However, it often becomes noticeable weeks to months later as the displacement accumulates. Immediate post-injection swelling can mask early migration, which is why delayed presentation is common.
Yes. Once the migrated filler is precisely removed from the shelf area, the lip contour typically returns to its natural shape. The vermillion border becomes defined again, and the upper lip loses its characteristic 'sausage' or 'duck' appearance. Many patients choose conservative re-injection 2-4 weeks after correction.
Absolutely. Nasal filler migration—often called 'Avatar nose'—responds very well to ultrasound-guided selective removal. We can reduce the spread product from the lateral nasal walls while preserving any desired dorsal height, restoring the nose to a natural width.
The 'shelf' or 'caterpillar' ridge above the lip border is filler that has migrated into a tissue plane that enzyme injections often don't reach effectively. Blind dissolution tends to dissolve the filler in the lip proper (the volume you wanted) while leaving the migrated product in the shelf untouched. Ultrasound-guided treatment can selectively target the shelf while preserving your lip volume.
Adding more filler to counteract migration rarely works and often makes the problem worse. You're adding volume to a system that already has too much in the wrong places. The displaced filler needs to be removed, not compensated for. More product means more hydrostatic pressure, which can actually drive further migration.
Completely different. Dissolution removes filler indiscriminately — destroying the good volume along with the bad. At FILLER REVISION, we use ultrasound to see exactly where the migrated product is, then selectively extract only the displaced portion while preserving what's in the right position. We're not dissolving everything and starting over — we're surgically precise about what stays and what goes.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then add LINE @liusmed with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.
In your LINE message, mention you posted in the FillerRescue forum.
References
- Schelke L, et al. Post-Treatment Displacement of Facial Soft Tissue Fillers — A Retrospective Ultrasound-based Investigation of 382 Zygomatic Regions. Dermatol Surg. 2024;50(10):946-952.
- Chae SY, et al. A Case of the Migration of Hyaluronic Acid Filler from Nose to Forehead Occurring as Two Sequential Soft Lumps. Ann Dermatol. 2016;28(5):645-647.
- Requena L, et al. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1-34.
Related Real Cases
Documented ultrasound-guided extraction and rescue cases by Dr. Ta-Ju Liu.


The information on this website is for educational purposes only and does not constitute medical advice. Individual results may vary depending on personal conditions; actual outcomes cannot be guaranteed. All medical procedures carry potential risks and complications. Please consult a qualified physician before making any treatment decisions.
Featured Poster
Three rounds of dissolving. The lump is still there.
60% of our patients arrive after repeated failed treatments elsewhere. When dissolvers fail, physical extraction is the main answer.